
Understanding Knee Osteoarthritis
Osteoarthritis (OA) is the most common degenerative joint disease, and the knee is its most frequent target. It is not simply “wear and tear” — it is a complex, progressive breakdown of the entire joint environment, involving cartilage, bone, synovial membrane, ligaments, and the muscles around the joint.
Stages of Knee OA (Kellgren–Lawrence Grading Scale):
- Grade I (Doubtful): Minimal joint space narrowing; small osteophytes (bony spurs) may begin to form. The patient may feel occasional stiffness but little pain.
- Grade II (Mild): More definite osteophytes; slight joint space narrowing. Pain begins to appear, especially after activity.
- Grade III (Moderate): Multiple osteophytes, definite joint space narrowing, some bone hardening (sclerosis), and possible bone-end deformity. Pain is more frequent and begins to affect daily activities.
- Grade IV (Severe): Large osteophytes, severe joint space narrowing, significant sclerosis, and definite bone-end deformity. Constant pain and significant disability.
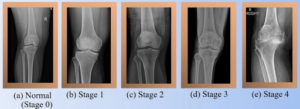
Image: The four stages of knee osteoarthritis showing progressive joint space narrowing and osteophyte formation (Kellgren–Lawrence Grade I–IV)
What Changes Inside the Knee in OA?
As OA progresses, several structural changes occur:
- Cartilage breakdown: The smooth articular cartilage that cushions the joint gradually wears away. This leads to bone-on-bone contact, causing pain and stiffness.
- Subchondral bone changes: The bone underneath the cartilage becomes thicker and denser (sclerosis) and may develop small fluid-filled cysts.
- Osteophyte formation: Bony spurs grow at the joint margins as the body tries (unsuccessfully) to stabilize the joint.
- Synovial membrane inflammation: The inner lining of the joint (synovial membrane) becomes inflamed, producing excess joint fluid — a key driver of pain and swelling.
- Capsular changes: The fibrous joint capsule becomes thickened, fibrotic, and contracted, restricting movement and adding to pain.
- Muscle wasting: The muscles supporting the knee — particularly the quadriceps — weaken over time due to pain-related disuse, further destabilising the joint.
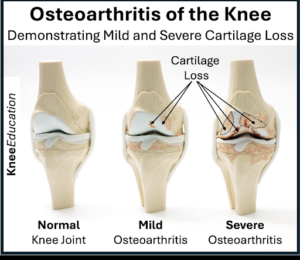
Image: Comparison of a healthy knee joint versus an osteoarthritic knee showing cartilage loss, osteophytes, and bone-on-bone contact
How and Why OA Causes Pain
Pain in OA is multifactorial. It does not come from cartilage alone (cartilage has no nerve supply), but from multiple pain-generating structures around the joint:
1. Hilton’s Law and Capsular Pain
Hilton’s Law states that the nerves supplying the muscles acting over a joint also supply the joint capsule and the skin over the joint. In OA, as the joint capsule becomes thickened and fibrotic, nerve endings within the capsule become sensitised — generating persistent, deep, aching pain with movement and even at rest. The capsular changes in OA are progressive and directly correlate with worsening pain.
2. Synovial Membrane Changes
The synovial membrane in OA undergoes significant transformation. Normally, it produces synovial fluid for joint lubrication and nutrition. In OA, chronic low-grade inflammation causes the membrane to thicken and generate excess fluid (effusion), along with inflammatory mediators such as IL-1β, TNF-α, and prostaglandins. These chemicals sensitise local nerve endings, contributing to pain, warmth, and swelling. The inflamed synovium is one of the primary pain generators in OA.
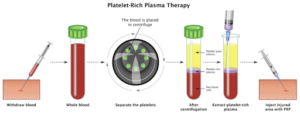
Image: Anatomy of the knee joint showing the synovial membrane, joint capsule, and surrounding structures — all pain-generating sites in OA
3. Periarticular Muscle and Trigger Point Pain
In addition to the joint itself, the muscles around the knee develop trigger points — hypersensitive knots within the muscle fibres — due to altered biomechanics, weakness, and compensation patterns. This myofascial pain component is often overlooked but is a significant contributor to overall knee pain in OA.
The Key Point: What Regenerative Therapy Can and Cannot Do
Regenerative therapy — including PRP and stem cell injections — is fundamentally designed to promote healing of damaged joint structures. It targets cartilage repair, reduces intra-articular inflammation, and slows disease progression.
However, it is important to understand that regenerative therapy addresses the structural damage within the joint — it does not specifically target the myofascial pain (trigger points, muscle changes, and capsular sensitisation) that has built up over months or years of disease. This is why, even after regenerative therapy, patients often report only 30–40% improvement in pain.
The remaining pain — arising from muscle trigger points, sensitised capsular nerves, and periarticular structures — needs to be addressed separately through Ultrasound-Guided Dry Needling (USGDN), a targeted, precise technique that deactivates trigger points and resets the pain cycle.
This is the foundation of our approach at Ashirvad Clinic: we treat the pain and the disease simultaneously — USGDN for pain relief and regenerative therapy for healing.
Knee pain can make even simple activities like walking, climbing stairs, or sitting uncomfortable. While traditional treatments such as painkillers, physiotherapy, or surgery are commonly used, many people are now exploring regenerative therapy as a newer, less invasive option.
But is regenerative therapy truly effective for knee pain? Let’s understand this in a clear and practical way.
What Is Regenerative Therapy?
Regenerative therapy is a modern medical approach whose primary goal is healing damaged tissues — not simply reducing pain. It works by stimulating the body’s own repair system to restore joint health at a biological level.
The most commonly used regenerative treatments for knee pain include:
1. Platelet-Rich Plasma (PRP) Therapy
A small sample of your blood is drawn and placed into a specialised centrifuge tube containing a separator gel. During centrifugation (typically at 1,500–3,000 rpm), the blood components separate by density. Red blood cells and pro-inflammatory white blood cells are retained below the separator gel, while the upper layer — rich in platelets and plasma — is collected as PRP.
This concentrated PRP contains powerful growth factors including:
- PDGF (Platelet-Derived Growth Factor): Stimulates cell growth and tissue repair
- TGF-β (Transforming Growth Factor-Beta): Promotes cartilage matrix production
- VEGF (Vascular Endothelial Growth Factor): Encourages new blood vessel formation
- IGF-1 (Insulin-Like Growth Factor-1): Supports chondrocyte (cartilage cell) function
Once prepared, the PRP is injected directly into the knee joint under sterile conditions. The growth factors are released and begin initiating a localised healing response — modulating inflammation, promoting tissue repair, and potentially protecting remaining cartilage.
Leukocyte-poor PRP (low in white blood cells) has been shown to be particularly effective for intra-articular use, as it minimises post-injection inflammation while maximising the regenerative signal.
Image: The PRP preparation process — from blood draw to centrifugation to concentrated platelet-rich plasma injection into the knee
2. Stem Cell Therapy
Special regenerative cells — mesenchymal stem cells (MSCs) — are harvested from your own body, most commonly from bone marrow or adipose tissue (body fat), and injected into the knee joint to help repair damaged cartilage and tissues.
A note on adipose-derived MSCs (Fat Mesenchymal Stem Cells):
Adipose tissue is an exceptionally rich source of mesenchymal stem cells. Fat-derived MSCs are harvested through a minimally invasive lipoaspiration procedure and are available in far greater numbers per unit volume compared to bone marrow-derived cells. Once extracted, these cells are processed and concentrated before being injected into the knee.
The Double Benefit of Adipose-Derived Stem Cell Therapy:
What makes adipose-derived stem cell therapy particularly exciting is its dual therapeutic mechanism:
- Reduces adipose tissue: The harvesting of fat during the procedure itself reduces localised adipose deposits. In patients who are overweight, excess adipose tissue contributes to the release of pro-inflammatory adipokines that worsen joint inflammation. Reducing this tissue can therefore have a direct anti-inflammatory benefit.
- Promotes joint healing: The injected MSCs migrate to the site of cartilage damage, where they release potent anti-inflammatory and regenerative signals, support cartilage repair, and modulate the immune environment within the joint.
This makes adipose-derived stem cell therapy a uniquely holistic treatment — it addresses both the systemic metabolic contribution to OA and the local joint damage simultaneously. For eligible patients, we strongly advocate for adipose-derived stem cell therapy as a premium regenerative option.

Image: Adipose-derived mesenchymal stem cells harvested from fat tissue and injected into the knee to promote cartilage repair and reduce inflammation
3. Prolotherapy
A natural irritant solution (commonly dextrose-based) is injected into the joint and surrounding ligaments to trigger a controlled healing response. This stimulates collagen production and helps strengthen lax or weakened ligaments around the knee.
How Does It Work?
Regenerative therapies aim to:
- Initiate a controlled inflammatory healing response — It is important to understand that regenerative therapies (particularly PRP) work by initially increasing local inflammation, not suppressing it. This acute, controlled inflammatory response is the trigger for the body’s natural repair cascade. This is fundamentally different from steroid injections, which suppress inflammation and may actually accelerate cartilage breakdown over time.
Promote tissue and cartilage repair
- Improve joint lubrication — While this is often claimed as a benefit, it must be noted that solid, high-quality evidence specifically for lubrication improvement remains limited. PRP may support the quality of synovial fluid indirectly through its anti-inflammatory effects, but this should not be overstated.
- Enhance mobility and function — However, a critical point must be acknowledged here: unless the pain component of OA is systematically addressed — specifically the myofascial trigger points, capsular sensitisation, and periarticular muscle pain — achieving meaningful improvement in mobility and function is extremely difficult, regardless of how well the joint is healing.
At Ashirvad Clinic, we address this limitation directly. We use Ultrasound-Guided Dry Needling (USGDN) to precisely target and deactivate myofascial trigger points around the knee, providing effective, lasting pain relief. Only when the pain is adequately managed can patients truly benefit from the mobility and functional improvements that regenerative therapy offers.
Unlike painkillers, which only provide temporary symptomatic relief, regenerative treatments attempt to address the root structural cause of the problem.
Is Regenerative Therapy Effective for Knee Pain?
What the Latest Evidence Says (2025):
PRP Therapy:
- A comprehensive narrative review published in the Journal of Clinical Medicine (2025), synthesising 40 high-quality studies including RCTs, systematic reviews, and meta-analyses, found that PRP injections — particularly leukocyte-poor PRP — demonstrate superior pain relief and functional improvement compared to hyaluronic acid and corticosteroids, especially in patients with mild to moderate OA (Kellgren–Lawrence grades I–III).
- A 2025 meta-analysis by Bensa et al., published in the American Journal of Sports Medicine, found that PRP offers clinically relevant functional improvement at 1, 3, 6, and 12 months, and significant pain relief at 3 and 6 months compared with placebo. Notably, higher platelet concentration was associated with superior and more durable outcomes.
- A 2025 meta-analysis by Li et al. (published in Open Access Journal of Sports Medicine), including 15 double-blind RCTs with 1,632 patients, demonstrated that PRP produced significantly lower WOMAC pain scores at 12 months compared to hyaluronic acid, with results exceeding the minimal clinically important difference.
- A prospective cohort study published in Cureus (October 2025), involving 113 patients with Kellgren-Lawrence grade 1–2 OA, confirmed significant improvements in pain (VAS) and function (WOMAC) following PRP injections with a favourable safety profile.
- An ongoing Phase 2 randomised double-blind controlled trial at the University of California San Francisco (UCSF) (2026) is currently investigating the protein and biological changes following PRP injections in knee OA, further underlining the growing scientific investment in this therapy.
Stem Cell / MSC Therapy:
- A systematic review and meta-analysis published in Frontiers in Cell and Developmental Biology (December 2025), covering RCTs up to October 2025, confirmed significant pain reduction on VAS across all timepoints following MSC therapy, with the strongest effects observed at 24 months — supporting a sustained, long-term benefit.
- A large prospective two-year case series of adipose-derived MSC therapy (329 patients) found that treatment was well tolerated with no serious adverse events, and all participant groups reported clinically and statistically significant pain improvement — with the potential to delay total knee replacement.
- A two-year prospective evaluation of MSC therapy published in the European Society of Medicine (June 2025) found significant early functional improvements, with Berg Balance Scale and WOMAC scores improving substantially from baseline.
The Bottom Line: The evidence consistently supports regenerative therapy — particularly PRP — for early to moderate knee OA. Results are most favourable in Kellgren–Lawrence grades I–III. However, it is important to be clear: these improvements are primarily in function and joint health, and the degree of pain relief from regenerative therapy alone is typically 30–40%. For complete pain management, a targeted approach to the myofascial and periarticular pain is also required.
However:
- Results vary from person to person. At Ashirvad Clinic, we believe this variability exists largely because regenerative therapy alone does not address the myofascial pain component. When we combine USGDN (for targeted pain relief) with regenerative therapy (for healing), outcomes are more consistent and complete.
- It may not work well in severe joint damage or advanced arthritis (Kellgren–Lawrence grade IV).
- Multiple sessions may be required for best results.
Benefits of Regenerative Therapy
- Minimally invasive — no major surgery required
- Uses your body’s own healing ability — autologous (your own cells/blood), so rejection risk is minimal
- Faster recovery compared to surgical procedures
- Lower risk of side effects
- Disease-modifying potential — unlike painkillers, these therapies aim to slow or partially reverse the underlying joint damage
At Ashirvad Clinic, we recommend a combined treatment approach:
- Ultrasound-Guided Dry Needling (USGDN) — for targeted, precise pain relief addressing trigger points, capsular sensitisation, and periarticular muscle pain
- Regenerative Therapy (PRP / Stem Cell) — for joint healing, cartilage protection, and long-term disease modification
This combination gives our patients both immediate pain relief and long-term healing — something neither treatment can reliably deliver alone.
Limitations and Considerations
- Treatment can be costly and is not always covered by insurance
- Results are not guaranteed and vary between individuals
- Requires skilled and experienced specialists for optimal outcomes
- Stem cell therapy remains under ongoing research in many regions, and protocols continue to evolve
- Regenerative therapy alone provides only partial pain relief (~30–40%); pain management must be addressed in parallel
At Ashirvad Clinic, we address these limitations by combining USGDN with regenerative therapy — ensuring pain is specifically and systematically treated, while the healing process is simultaneously supported.
Who Is the Right Candidate?
You may benefit from regenerative therapy if you:
- Have chronic knee pain due to OA or injury
- Have not found adequate relief with medications or physiotherapy
- Want to delay or avoid knee replacement surgery
- Are in the early or moderate stage of joint degeneration (KL Grade I–III)
- Are motivated to address both pain and healing with a comprehensive treatment plan
When Is It Not Enough?
Regenerative therapy may not be sufficient if:
- There is severe cartilage loss (bone-on-bone arthritis)
- The knee joint is significantly deformed
- Kellgren–Lawrence Grade IV OA is present
In such cases, surgical options including partial or total knee replacement may still be necessary. Your specialist will guide you appropriately.
Frequently Asked Questions (FAQs)
1. Is regenerative therapy safe?
Yes. Most treatments are considered safe as they use your own body’s cells and blood components. They should always be performed by qualified, experienced specialists under sterile conditions.
2. How long does it take to see results?
Improvement in function usually begins within a few weeks. Full regenerative benefits typically develop over 2–3 months as the healing cascade progresses.
3. Is the procedure painful?
Discomfort is minimal and temporary. Most procedures are performed under local anaesthesia or with ultrasound guidance to ensure accuracy and comfort.
4. How long do the results last?
PRP results can last 12–24 months, often significantly longer than steroid injections. Stem cell therapy may provide benefits for 2 years or more. Combining with USGDN optimises long-term outcomes.
5. Why do I need USGDN along with regenerative therapy?
Because regenerative therapy heals the joint but does not specifically address the muscular trigger points and periarticular pain that have developed over years of OA. USGDN precisely targets these pain generators — ensuring you get both pain relief and healing.
Final Verdict: Is It Worth Trying?
Regenerative therapy is a promising, evidence-backed, and evolving treatment for knee osteoarthritis. It works best for patients in the early to moderate stages of joint damage, offering real potential to slow disease progression and reduce the need for surgery.
However — and this is critical — regenerative therapy alone is not a complete solution for knee pain. The pain component of OA, arising from myofascial trigger points, capsular sensitisation, and periarticular changes, must be addressed separately and systematically.
At Ashirvad Clinic, our unique combined protocol of USGDN + Regenerative Therapy ensures that we are treating both the pain and the disease — giving our patients the best possible outcome.
Conclusion
If you are struggling with knee pain and looking for alternatives to surgery, regenerative therapy is absolutely worth considering — but only as part of a comprehensive treatment plan. Healing the joint while ignoring the pain is an incomplete approach.
At Ashirvad Clinic, we believe in treating the whole picture — combining Ultrasound-Guided Dry Needling for precise pain relief with Regenerative Therapy for long-term healing. Consult our specialist team to find out if this combined approach is right for you.





