
Osteoarthritis of Knee (OA knee) occurs because of age related degeneration causing damage to the knee and is one of the most common causes of pain and disability in the world. As such OA knee places a huge health related burden on individuals and the healthcare system and society because even simple activities like walking, climbing stairs, or sitting become uncomfortable.
| Worldwide | About 375 million people live with knee arthritis today. Roughly 30 million new cases appear each year and the number keeps rising. |
| Countries with most number of cases | China has the most cases, followed by India and then the United States. |
| India | Knee arthritis is the most common form of arthritis here. Community studies find that roughly 1 in 4 to 1 in 3 adults (about 22–39%) have it — more often women. |
Patients are often confused about which treatment is best suited for them so that their pain and disability is reliably relieved, enabling them to resume a normal life.
The treatments for osteoarthritis of the knee address three main problems. All these treatments have different goals.
- Surgery- targets the structural problems by replacing the knee damaged by arthritis.
- Non-surgical options – are pain management and regenerative therapies. The goals of these two treatments are very different.
- Pain management treatments – primarily address the pain and disability and indirectly create a situation where the joint function is optimized. Here the patient definitely achieves pain relief and therefore disability relief, but degeneration reversal is a secondary goal which might be partially achieved.
- Regenerative therapies, primarily address the inflammation and attempt to reverse the degenerative changes of arthritis. Growth factors are injected into the joint either in the form of platelet rich plasma or growth factor concentrate harvested from blood, fatty tissue or the bone marrow. They all target regeneration of the damaged joint and have shown significant improvement on MRI pain and functionality. However, the goal of the regenerative therapy is primarily healing and pain relief comes as a consequence of the healing. As a result, there may be no significant pain relief for weeks or months after regenerative therapy. Being secondary goals they might be achieved partially or might not be achieved to the patient’s satisfaction.
Since the 2 noninvasive treatment options address different problems it would be best to combine pain management and regenerative therapies. The pain and disabilities should be relieved first so that the patient becomes comfortable and then regenerative therapies undertaken.
Surgery: replaces the diseased knee joint with an artificial one. On the face of it, it looks like the best solution but in practice it is not indicated in all patients because it involves the risk of major surgery requiring anesthesia, followed by painful rehabilitation which might prove to be difficult for many patients. Post surgical complications like neuropathy might occur as the body’s reaction to the surgery despite a perfectly performed surgery by a skillful surgeon. Because of these risks a good surgeon will never recommend surgery unless structural damage definitely indicates surgery.
Surgery is indicated when the structural damage to the knee is considerable, usually classified by a scale called Kellgren-Lawrence scale. Grade 3 and 4 indicate a definite need for surgery and many of these patients do well only after surgery.
OSTEOARTHRITIS · RADIOGRAPHIC GRADING
Kellgren–Lawrence Grading Scale
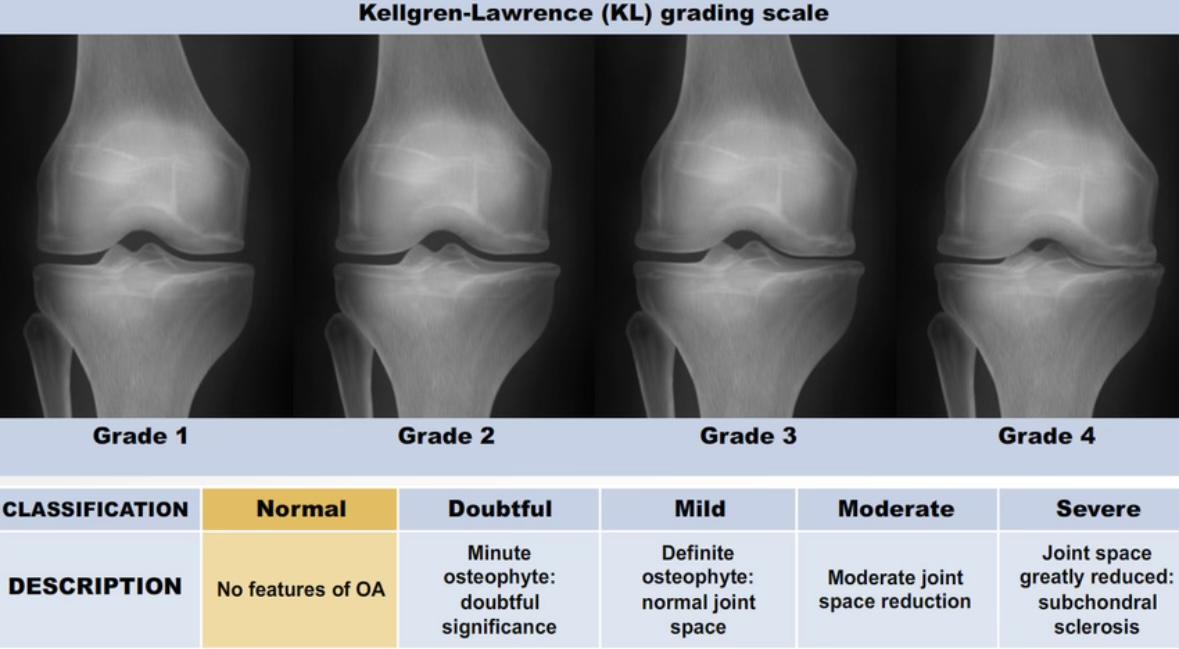
Grade ≥ 2 is the radiographic threshold for definite OA — the defining feature is a definite osteophyte.
Severity sequence: osteophytes → joint-space narrowing → subchondral sclerosis → bony deformity.
Always grade on weight-bearing films; non-WB views underestimate joint-space narrowing.
Most widely used OA grading system — described 1957, WHO-adopted 1961.
Limitation: osteophytes are weighted heavily, so early cartilage loss may be under-graded (cf. OARSI, Ahlbäck).
How many knee replacements are done each year?
| United States | Around 600,000 to 1 million knee replacements a year — one of the most common major operations. Expected to keep growing. |
| Europe | Rates vary a lot by country. The highest are in Switzerland and Finland (about 260–270 per 100,000 people each year). Across the major Western nations, surveys count over a million procedures yearly. |
| India | About 200,000 knee replacements a year (2020 estimate), and growing fast. Almost all are done for arthritis. |
| Worldwide | About 3.6 million knee replacements a year, with the US doing nearly 40% of them. |
How often do problems happen after surgery?
Most people do well. Studies usually report problems at 1 month (“early”) and at 3 months — there isn’t a separate widely-used “6-month” figure, so the 3-month number is the best guide for the months after surgery.
| Early (first month) | About 3 to 6 out of every 100 patients have some complication. Risk of death is very low — well under 1 in 100. |
| Later (by 3 months) | Roughly 3 to 5 out of every 100 patients, lower when patients are carefully prepared beforehand. |
Nerve damage after surgery (neuropathy)
Nerve injury is rare. The main nerve at risk is the common peroneal nerve. It happens in about 3 to 4 out of every 1,000 operations (0.3 – 0.4%). The risk is higher — around 2 in 100 — in knees that are badly bent inward/outward before surgery. Most patients recover
Summary of Post-TKR Complications
| Persistent pain (CPSP) | Stiffness / arthrofibrosis | Infection (PJI) |
| Commonest complaint and main cause of dissatisfaction. ~10–34% have significant chronic pain; ~20% dissatisfied. Often neuropathic — about half of chronic-pain cases screen positive. | Restricted ROM from intra-articular adhesions and fibrosis. A leading early cause of re-operation — manipulation under anaesthesia or arthrolysis. | Most feared complication. Early (<3 mo), delayed low-grade, or late haematogenous. Managed by DAIR or single/two-stage revision. |
| Mechanical / implant | Patellofemoral & extensor | Neurovascular & systemic |
| Aseptic loosening (leading late-revision cause), polyethylene wear and osteolysis, instability, periprosthetic fracture, component malalignment. | Patellar maltracking, anterior knee pain, patellar clunk, component failure, and extensor-mechanism / tendon rupture. | Common peroneal palsy (most disabling), saphenous / IPBSN injury (commonest cutaneous), CRPS; plus VTE, wound necrosis, anaemia. |
55–84% of patients show IPBSN sensory disturbance after TKA
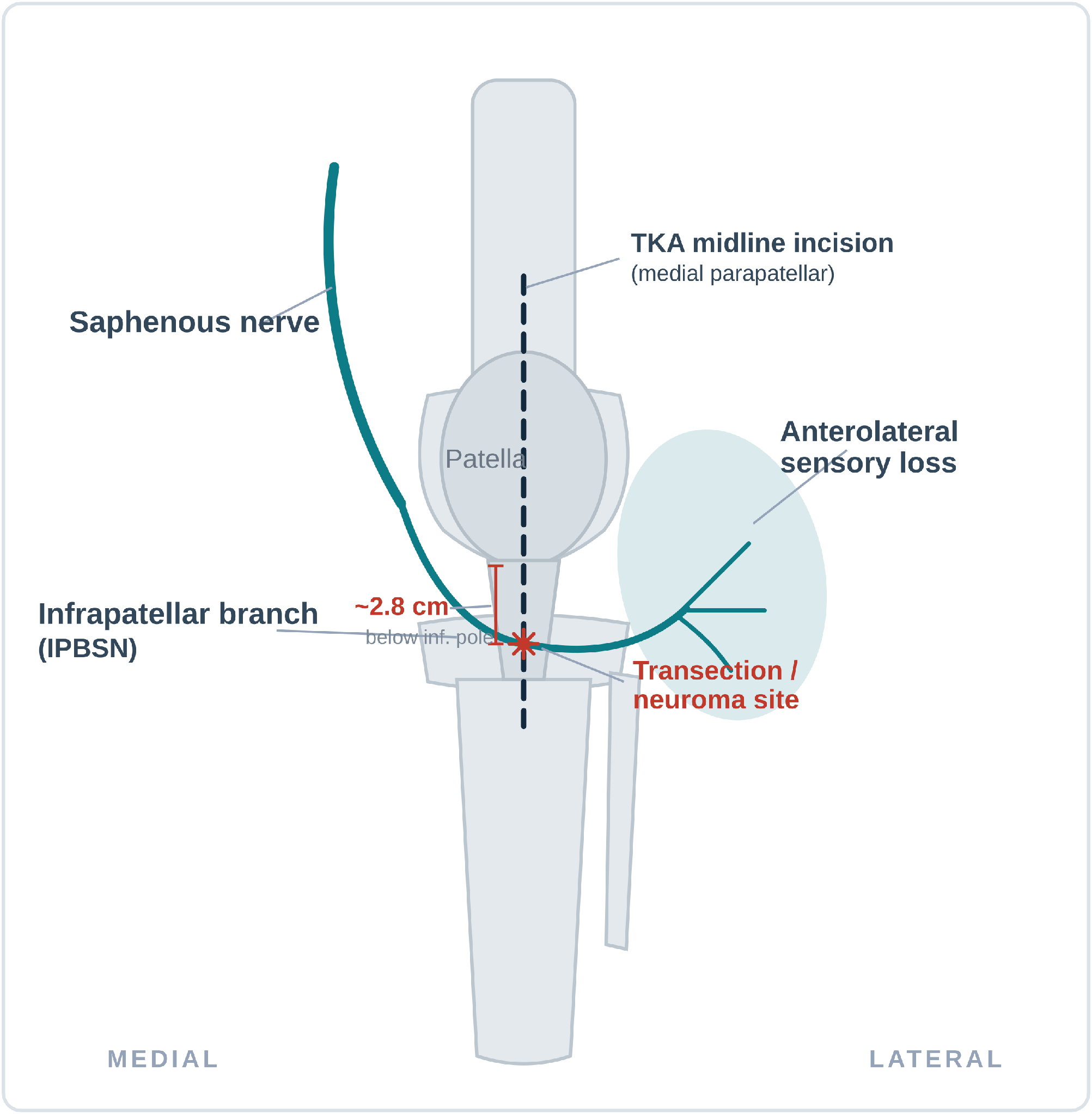
| Mechanism | Presentation |
| The standard midline / medial parapatellar incision crosses the transverse IPBSN ~2.8 cm below the inferior patellar pole → transection, painful neuroma, or scar entrapment. | Numb / dysaesthetic patch lateral to the scar; burning or stabbing anteromedial pain; positive Tinel’s sign; allodynia to kneeling that can limit flexion. |
| Diagnosis | Management |
| Clinical — exclude infection, loosening, instability, referred pain. Diagnostic IPBSN LA block (>50% VAS drop) confirms source and predicts response; USG / MRI localise neuroma. | Step-up: neuropathic agents + desensitisation → LA ± steroid, hydrodissection, pulsed RF / RFA, cryoablation, PNS → neurolysis / selective neurectomy. ~70% full relief. |
Patients who are better off with non-surgical treatments
Patients with grade 2 and some patients with grade 3, do not require a replacement because the natural joint can sustain weight-bearing and its functionality quite well, much better than any artificially replaced joint. However, many grade 1-2 patients have significant amount of pain even though the OA is in its early stages but pain itself should not be an indication for surgery unless there is significant joint damage, So, in early OA knee where the joint degeneration /damage is not advanced, newer, less invasive conservative treatments are better options.
While traditional treatments such as painkillers, physiotherapy are commonly used, they have a ceiling effect in that the pain relief reaches a particular level and then will not go further. For example, if a patient has severe pain (8—9 on a scale of 1-10, and can walk only 10 minutes with some difficulty and is given pain killers and physiotherapy for a month. There may be different results in different people. In some fortunate few, the pain may gradually go down steadily and the patient steadily but very gradually regains the ability to walk longer and longer and reach a level where they can walk about 30-40 minutes comfortably. These patients do not need any further treatment but can simply continue physiotherapy and take medications on an as needed basis. A word of caution here;
Even if the pain goes down at rest, if they cannot increase the duration of walk or are unable to climb 2-3 flights of stairs after 1-2 months of physiotherapy, they need pain management and regenerative therapy. It is important to know when the ceiling effect of pain and disability relief has been reached, and they need to look for a more useful treatment that fulfills the goal of painless walking for 40-60minutes and the ability to climb 2-3 flights of stairs comfortably. There is no point in continuing only physiotherapy alone if the progress has come to a halt. Anyway, medications and physiotherapy will continue as a part of their treatment even after pain management and regenerative therapies are initiated.
But in a majority of patients, just medications and physiotherapy pain may go down to 6-7 /10 and they may walk about 10-14 minutes at this lower pain level, but thereafter the relief stagnates and the patient cannot progress further even after a month, It is time for these people who should seek pain management and regenerative therapies because pain management works at a completely different level to ensure definite pain relief and healing.
In addition to patients with structural changes of Kellgren Lawrence grade 1 and 2, there are other categories of patients who opt for the combination of pain management and regenerative therapies.
Patients who cannot have surgery
There is no single reliable global number for this. Some patients are not suitable because of other health problems (heart disease, uncontrolled diabetes, severe obesity, frailty due to old age). In real-world studies, only a small share of people who need a knee replacement actually receive one — for example, just about 6 in 100 eligible patients had surgery within 18 months in one study — but these mix “unfit” with “can’t get access.”
Patients who say no to surgery
This varies a lot by country and age. When surgery is offered or recommended, somewhere between about 15% and 30%+ of suitable patients choose not to have it. Willingness also drops over time and with older age.
People waiting for surgery in the UK
| Bone & joint waiting list | Almost 860,000 people were waiting for bone and joint (orthopaedic) treatment in England (Oct 2025) — the largest waiting list of any specialty. |
| Typical wait | Around 28–29 weeks (about 7 months) for a knee replacement in 2025. |
| Overall NHS backlog | About 7.3 million treatments were waiting (roughly 6.2 million people) in late 2025. |
Pain management therapies – Unlike painkillers, which only provide temporary relief, these treatments produce long term pain relief allowing the patients to become better with physiotherapy specifically target and relieve the pain and disability. Most pain clinics in India and abroad perform radio frequency (RF) procedures and then refer patients to physiotherapy. Ashirvad protocol is different from most other pain clinics where the most commonly performed procedure is ablation of the nerve that supplies sensation to the joint called genicular nerves. These are small nerves dedicated to the joint for joint sensation and pain. Since they are exclusive to the joint, these nerves can be ablated by applying heat at 70-80°C to them(thermal RF). Alternatively there is a procedure called cooled RF where the RF probe is cooled by circulating water channels around it so that heat is delivered at 600 and is claimed to have better results at achieving a cessation of pain conduction by the nerves. This thermal or cooled RF is aimed at relieving only the pain from the joint. This is followed by physiotherapy to rehabilitate these patients and achieve functionality
Conventional RF vs Cooled RF
Genicular nerve radiofrequency ablation for knee osteoarthritis — success rates
“Success” = at least 50% pain relief, the standard measure used in these studies.
Success rates at a glance
| Measure | Conventional RF | Cooled RF |
|---|---|---|
| Short-term success | 59–64% | 65–77% |
| Best single-study figure | 64% at 6 months | 76.5% at 3 months |
| Lasts up to 2 years? | long-term data is Limited | Yes — ~63% at 24 months |
| Vs placebo (sham) | — | 76.5% vs 33.3% |
Cooled RF — how long it lasts
| Time after procedure | Patients still with ≥50% relief |
|---|---|
| 12 months | 65% |
| 18 months | 69% |
| 24 months | 63% |
Source: prospective multicentre trial.
Head-to-head: is cooled RF better?
| Time point | Odds favouring Cooled RF | Statistically certain? |
|---|---|---|
| 1 month | 1.46× | No |
| 3 months | 2.38× | No |
| 6 months | 2.70× | No |
Cooled RF scored higher at every point, but there was only one direct comparison trial that was small in numbers, so the difference was not proven (could be chance). So both types of work; cooled tends to score higher and last longer.
Reality check
The figures above are from carefully selected patients. In everyday practice, results are lower: in one real-world group pain improved in 71%, but only 26% reached the “half the pain gone” mark. Good patient selection strongly affects success.
At Ashirvad Institute of Pain Management, we take a different approach. We believe that disability relief is as important as pain relief and specifically work towards relieving both pain and disability with the goal that patients should walk 30-45 minutes without pain and climb 2 flights of stairs. We believe that the pain in osteoarthritis of the knee is not just coming from the joint, but mainly from the muscles around the joint. This is because the joint and the muscles that move the joint are intimately connected by a physiological law called Hilton law, which states that the highly innervated synovium (inner lining of the joint and the capsule of the joint) is intimately connected to the muscles that move the joint. As a result, any inflammation in the joint as in arthritis causes a lot of muscle spasm, which is the cause of all knee pains
So we address the nerves that supply all the muscles of the joint with an RF procedure called pulsed radio frequency (PRF) where the nerves are not burnt or ablated. The radio frequency energy is applied at 42°, which is a very safe temperature for the nerves which are designed by nature to withstand similar temperatures in high fever where the core temperature goes to 42°C. So, the nerves can withstand this 42 °C temperature of PRF very well without showing any negative effects. But only the thinner C and A delta nerves that are dedicated to carrying pain undergo targeted change to produce pain relief and muscle relaxation.
The PRF is applied to all the nerves that supply the muscles responsible for knee movements such as,
1.The femoral nerve that supplies all the 4 quadriceps muscles the skin of front of the thigh and knee,
- The sciatic nerve that supplies the hamstring muscles at the back of the knee, the calf muscles and all the muscles of leg and foot,
- The saphenous nerve that supplies an important and painful muscle called sartorius which along with the inner hamstring and gracilis muscle forms the Pes anserine tendon which is responsible for the pain on the inner side of the calf below the knee.
PRF also addresses 3 nerve plexuses that innervate the knee itself, such as the
- Prepatellar plexus responsible for all the sensations around the patella (knee cap)
- Subsartorial plexus – responsible for all the sensations in the inner
side of knee
- The popliteal plexus responsible for all the sensations at the back of the knee
- The 4 genicular nerves that carry knee joint sensations
We occasionally resort to addressing the genicular nerves with thermal ablation in K_L grade 3-4 patients who either cannot have surgery due to medical conditions or refuse to have the surgery.
In addition to PRF that relieves all the nerve pains, we also specifically address the Muscle pain stiffness and disabilities with a treatment called ultrasound guided dry needling (USGDN)
This treatment targets the painful knots in all the muscles of the knee, back and hip and particularly the calf. As a result, most of the pains in these muscles disappear. Not only does the original pain disappear, the new pains that come because the patients are now walking and climbing stairs will also be relieved on a weekly basis till the patients develop the strength in all the muscles that had become deconditioned by the pain of arthritis. and also the muscle relaxes to become more flexible allowing more movements and better movement range. Muscle relaxation also allows the 2 main bones to move apart so that the friction and cartilage loss become less, and the patella which is usually pulled outwards by quadriceps muscle spasm returns to the center improving the mechanical advantage of the knee. Thus PRF + USGDN is not just a pain relief treatment but also produces structural improvement of the knee.
The comfort of a flexible knee and muscle pain relief by USGDN enables the patients to use their muscles more and more without pain to become functionally active by walking 40-60 minutes and climbing 2-3 flights of stairs.
Once the Patients have achieved this goal then we recommend regenerative therapy which can reverse the degenerative changes so that their knee can heal so that they avoid knee replacement
What Is Regenerative Therapy?
Regenerative therapy is a modern medical approach that focuses on healing damaged tissues naturally rather than just reducing pain. It works by stimulating the body’s own repair system.
The most commonly used regenerative treatments for knee pain include:
1. Platelet-Rich Plasma (PRP) Therapy
A small sample of your blood is processed to concentrate the growth factors (healing components) in the platelets which are then injected into the knee joint.
2. Stem Cell Therapy
Special cells are taken from your body (usually bone marrow or fat tissue) and injected into the knee to help repair damaged cartilage and tissues.
3. Prolotherapy
A natural solution of glucose is injected into the joint to trigger a healing response and strengthen ligaments.
How Does It Work?
Regenerative therapies aim to to address the root cause of the problem.:
– Reduce inflammation
– Promote tissue repair
– Improve joint lubrication
– Enhance mobility and function
Is Regenerative Therapy Effective for Knee Pain?
What the evidence suggests:
– Many patients experience moderate to significant pain relief
– It is especially effective in early to moderate osteoarthritis
– PRP therapy has shown promising results in clinical studies
– Improvement may last longer compared to steroid injections
However:
– Results vary from person to person
– It may not work well in severe joint damage or advanced arthritis
– Multiple sessions may be required for best results
Benefits of Regenerative Therapy
– Minimally invasive (no major surgery required)
– Uses your body’s own healing ability
– Faster recovery compared to surgical procedures
– Lower risk of side effects
Limitations and Considerations
– Treatment can be costly and not always covered by insurance
– Requires skilled and experienced specialists
– Stem cell therapy is still under ongoing research in many regions
– Results are not guaranteed in every patient but,
When combined with PRF of nerves and USGDN it becomes a comprehensive therapy for osteoarthritis.
PRF addresses joint degeneration
PRF addresses nerves that cause muscle spasm via Hiton’s law and also carry pain.
USGDN eliminates muscle knots and taut muscle bands to optimize muscle function and produce structural improvement of the joint
Who Is the Right Candidate?
You may benefit from regenerative therapy if you:
– Have chronic knee pain due to arthritis or injury
– Have not found relief with medications or physiotherapy
– Want to delay or avoid knee replacement surgery
– Are in the early or moderate stage of joint degeneration
When Is It Not Enough?
Regenerative therapy may not be suitable if:
– There is severe cartilage loss
– The knee joint is significantly deformed
– Advanced arthritis is present
In such cases, surgical options may still be necessary.
Final Verdict: Is It Worth Trying?
Regenerative therapy is a promising and evolving treatment for knee pain. It works best for patients in the early stages of joint damage and those looking for non-surgical options.
While it is not a miracle cure, it can significantly improve pain and function in the right candidates.
Conclusion
If you’re struggling with knee pain and looking for alternatives to surgery, a combination of regenerative therapy along with PRF and USGDN which has helped hundreds of patients at our clinic since 2006 is well worth considering.
Frequently Asked Questions (FAQs)
1. Is regenerative therapy safe?
Yes, most treatments are considered safe as they use your own body’s cells. However, they should always be performed by qualified professionals.
2. How long does it take to see results?
Improvement usually begins within a few weeks, with full benefits developing over 2–3 months.
3. Is the procedure painful?
Discomfort is minimal and temporary. Most procedures are done under local anesthesia.
4. How long do the results last?
Results can last from several months to a few years, depending on the condition and lifestyle factors.
Sources for knee arthritis
Global burden of knee osteoarthritis 1990–2021 (375 million cases; ~3 million annual). PLOS One, 2025. https://journals.plos.org/plosone/article?id=10.1371/journal.pone.0320115
Global burden of knee osteoarthritis — country ranking and ~30.85 million annual incidence (China, India, US). PMC, 2025. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11993502/
Burden of osteoarthritis in India, 1990–2019 (GBD 2019). Osteoarthritis and Cartilage, 2022. https://www.sciencedirect.com/science/article/pii/S1063458422007427
Epidemiology of knee osteoarthritis in India (prevalence 22–39%; 28.7%). PubMed, 2016. https://pubmed.ncbi.nlm.nih.gov/27746495/
Total knee replacement volume in the US (600,000+ annually). ClinicalTrials.gov protocol. https://cdn.clinicaltrials.gov/large-docs/75/NCT03434275/Prot_000.pdf
US knee replacement volume and 2030 projection (~3.5 million). The Center, 2022. https://www.thecenteroregon.com/medical-blog/knee-replacement-surgery-by-the-numbers/
Knee replacement rates by country, 2021 (Switzerland, Finland highest). Statista / OECD. https://www.statista.com/statistics/236586/number-of-knee-operations-in-selected-countries/
International survey of total knee replacement (18 countries; ~1.32 million procedures). PMC. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3224613/
India joining hip and knee registries (~200,000 in 2020; registry data). PMC, 2020. https://pmc.ncbi.nlm.nih.gov/articles/PMC8149501/
Global knee market — ~3.6 million procedures worldwide, US ~40%. LSI, 2024. https://www.lifesciencemarketresearch.com/insights/the-global-knee-market-insights-and-projections-for-2024-and-beyond
30-day complications and mortality after TKA (5.6%; 0.18%). PubMed, 2014. https://pubmed.ncbi.nlm.nih.gov/24382720/
Incidence and timing of complications after TKA (2.90% at 30 days). Canadian Journal of Surgery, 2024. https://www.canjsurg.ca/content/67/6/E377
90-day complications after TKA (5.3% vs 3.1% with preparation). PMC. https://pmc.ncbi.nlm.nih.gov/articles/PMC8858904/
Peroneal nerve palsy after TKA — systematic review (0.4%). PMC. https://pmc.ncbi.nlm.nih.gov/articles/PMC7451888/
Peroneal nerve injury after TKA (reported 0.3–4%). Journal of Medical Sciences, 2021. https://journals.lww.com/joms/fulltext/2021/41050/peroneal_nerve_injury_after_total_knee.6.aspx
Peroneal nerve palsy in valgus knees (1.9%). PMC. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC8776926/
Inequalities in access to knee replacement (6.4% of eligible operated in 18 months). PubMed, 2004. https://pubmed.ncbi.nlm.nih.gov/15479899/
Willingness to consider joint replacement (14% willing). PMC. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7275466/
Decision to receive TKR — 217 of 704 did not have surgery. Scientific Reports, 2024. https://www.nature.com/articles/s41598-024-81852-7
Patient preferences for TKR — 215 of 804 unwilling; willingness declines. Univ. of Arizona. https://experts.arizona.edu/en/publications/patient-preferences-for-total-knee-replacement-surgery-relationsh/
NHS waiting list — trauma & orthopaedics ~860,000 (Oct 2025). The King’s Fund. https://www.kingsfund.org.uk/insight-and-analysis/data-and-charts/waiting-times-non-urgent-treatment
Knee/hip replacement waiting times (28–29 weeks; 7.3 million backlog). Patient Claim Line, 2026. https://www.patientclaimline.com/article/knee-hip-replacement-waiting-times/
Sources for RF treatment details
Conventional RF of genicular nerves — 59% achieved ≥50% relief (Choi et al). ClinicalTrials.gov protocol. https://cdn.clinicaltrials.gov/large-docs/69/NCT02260869/Prot_SAP_000.pdf
Radiofrequency denervation for knee pain — evidence review (64% success at 6 months). BJA Education, 2024. https://www.bjaed.org/article/S2058-5349(24)00018-0/fulltext
Cooled RFA vs sham — 76.5% vs 33.3% responders at 3 months. Medicina (MDPI), 2024. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11206112/
Cooled RFA 24-month durability (65% / 69% / 63%). Pain Practice, 2022. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC9541208/
Cooled vs conventional RF head-to-head (COCOGEN trial). Reg Anesth Pain Med, 2023. https://pmc.ncbi.nlm.nih.gov/articles/PMC10086476/
Real-world genicular RFA outcomes (71% improved, 26% with ≥50% relief). 2023. https://www.researchgate.net/publication/367247271_Comparison_of_cooled_versus_conventional _radiofrequency_treatment_of_the_genicular_nerves_for_chronic_knee_pain_a_multicenter_non-inferiority_randomized_pilot_trial_COCOGEN_trial





