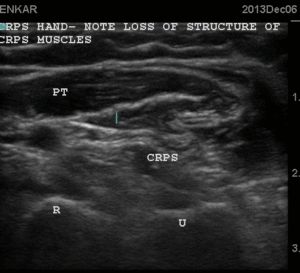
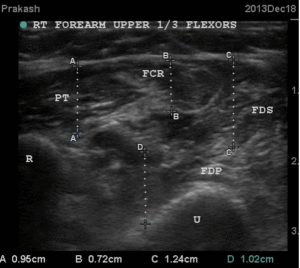
Figure 16 USG showing muscle regeneration at 12 days


Row 1:
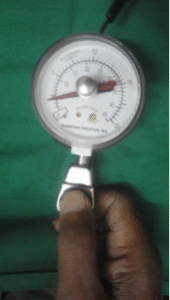
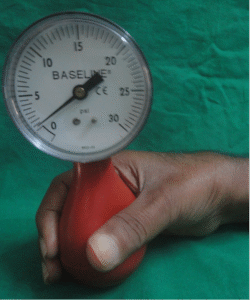
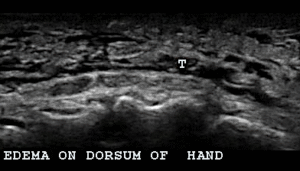
Right hand with CRPS swollen warm and painful cant bend the finges at all. Pinch gauge for finger shows very low pressure and dynamometer zero pressure.
Row 2:
The USG images on 6th December show that there are no clear outlines for muscles which are hyper echoic. The same hand on December 18th after 6 sessions of USGDN shows return of clear muscle outlines, with islands of hypoechoic muscle tissue in the hyperechoic fibrotic mass.
Row 3:
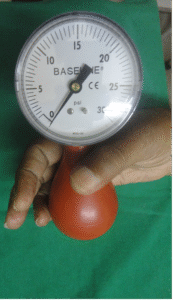
He is now able tp flex the fingers, generates 1 PSI pressure, is able to turn doorknobs and write legibly
This led to a lot of queries by the reviewers which had to be satisfactorily answered point by point, but the saving grace was that there were 31 pictures which told their own convincing story in irrefutable black and white. Even now in 2025, 12 years later, all the publications on this topic have come exclusively from the Ashirvad group. No other research group has explored the USG changes of muscle in CRPS either to refute or corroborate our findings, though it has been cited >32 times by different authors.
Another problem was the highly unusual nature of this topic which dealt with the potential of USG as a diagnostic investigation in CRPS where there had been no investigation to clinch the diagnosis. MRI as a diagnostic investigation had been proposed but was refuted shortly thereafter as being inconsistent. X-ray does show osteopenia and osteoporosis in later stages but by that time the diagnosis would have been already established.
The addition of USG into our armamentarium opened the door to the hitherto unexplored world of muscle pathology in CRPS which provided many answers to explain the enigma of not only CRPS but a related but much milder pathology of co-contraction, the writer’s cramp. (49-60,75)
How co-contraction explains the inflammatory symptoms and signs of CRPS:
Inflammation has always been cited in CRPS literature as an important finding (76) but never with reference to muscles. The inflammation has been attributed to nerves as a neuroinflammation to explain the increased levels of inflammatory mediators that have been demonstrated in the cerebrospinal fluid of CRPS patients as well as in the blood collected from the veins of CRPS limb as compared to the normal limb. The proposed explanation for this is that inflammation is supposed to involve the nervous system at all levels right from the spinal cord down to the peripheral nerves of hand and is supposed to express itself peripherally as the inflamed red swollen hand of CRPS. This concept of neuroinflammation neither acknowledges nor attempts to explain the muscle stiffness. Instead the stiffness and disability of the CRPS hand is attributed to the Central nervous system which somehow decides to “neglect” the CRPS hand and eventually joints of the hand get fused after a few years. However, neither the medications that address the nervous system ( neuromodulators) or the interventions that address this hypothetical neuroinflammation may or may not produce beneficial results. Nerve blocks (with injection of anti-inflammatory drugs like steroids) may not work at all or may relieve CRPS symptoms temporarily. We have seen that SGB works only in patients with sympathetically maintained pain but not in those with sympathetically independent pain. Single shot or short-term blocks of somatic nerves work temporarily. In our 40 patients with CBPB, the block had to be continuous 24/7 and maintained for 40-60 days for physiotherapy to be effective. Those patients with accidental extrusions at 10-15 days or earlier there was a full-blown recurrence of CRPS symptoms before we introduced USGDN as an additional treatment (after our east African patient in 2006). In retrospect it is obvious that once USGDN was introduced even those patients with accidental catheter extrusions within the first 2 weeks went on to recover completely from CRPS. This data indicates that the nerve blocks play a secondary role in addressing the CRPS symptoms, their effects confined to partial and temporary relief of only pain and sensory symptoms. Thus, neuroinflammation does not seem to comprehensively explain CRPS.
In contrast, the Ashirvad understanding explains that while the inflammation of hand is very real, it is not neuroinflamamtion from spinal nerves which somehow mysteriously expresses itself in the hand but is actually a localized tenosynovial inflammation consequent to involvement of muscles and their tendons.
CRPS patients have a very clear and specific description of their pain. They seldom complain of any significant pain in the forearm where the co-contracted muscles are but always point to their fingers and wrist as the painful areas. It was a perplexing observation to solve. So how and why does co-contraction of muscle in forearm produce pain in the fingers and why exactly does the relaxation of forearm muscle relieve the pain, swelling, redness and warmth of CRPS hand?
USG provided the answer by showing that the hand swelling in CRPS patients was actually a collection of fluid around the tendons(effusion) of the extensor muscles at the back of the hand. There is no swelling at all in the soft tissues of the hand superficial to the tendons. (figure-21). The flexor tendons in front of the hand and wrist are inflamed and USG shows effusion around these tendons as well but the swelling on dorsum(back) of hand is much more obvious.
Figure 17- Ultrasound appearance of the inflammation around tendons
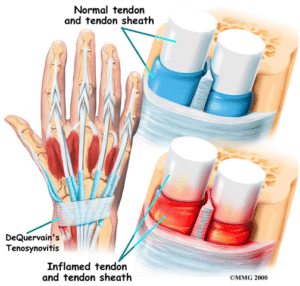
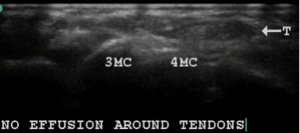
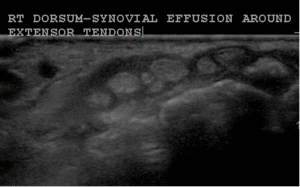
The first image shows the diagrammatic representation of tendons of the hand and the synovial covering around it. The 2nd image is from a non CRPS patient where the swollen hand shows collection of fluid under the skin (subcutaneous) as irregular black spaces but the tendons are normal. The 3rd image shows the collection of black fluid around the white round tendons in a CRPS patient while the subcutaneous tissues have no fluid. The 4th image shows the same patient after treatment where the effusion has disappeared and the tendons are normal.
The tendons of the flexor and extensor muscles of the fingers have a very thin covering (synovial sheath) with an extremely rich supply of nerves. Any overstretching/ pull/friction between the tendons and this sheath produces local inflammation called tenosynovitis. Once USG showed this tenosynovial effusion, I understood that the straining and struggling of co-contracted muscles with attempts to move the hand or make a fist causes repeated friction between the tendons and their tendons causing inflammation. (tenosynovitis) This releases inflammatory mediators which lead to increasing pain, warmth and swelling which can be visualized by USG around the tendons. This inflammatory tenosynovitis in turn reciprocally worsens the spasm of the already co-contracted flexor and extensor muscles which in turn worsens the pull on the tendons and further inflammation forming a vicious circle.
Exercises of the fingers and hand of CRPS feed into this vicious circle to increase the friction and hence the repeated exacerbations. It is as if the limb affected by CRPS-1 experiences a trauma every time the patient attempts physical therapy or tried to use the hand and hence experience an exacerbation of their symptoms when they did physiotherapy. It is also a common finding that patients have no symptoms of CRPS as long as their hand is immobilized in a plaster cast and the problems of pain and swelling start only during the mobilization phase after removal of plaster cast. They also complain that it is their fingers that hurt most and later swell, when they try to make a fist.
Pain during the needling appeared to vary directly with the resistance encountered by the needle in the CRPS muscles. This resistance is caused by intense co-contraction in the initial phases of CRPS and by fibrosis of muscle in later phases. Patients report that they are happy to cooperate for USGDN despite this pain because of the exquisite relief of their original pain after needle removal. Even more important to them is the returning ability to use the hand and the ability to sleep undisturbed by the pain. All of them comment on the difference in pain and movement restriction before and after DN.
The movement restriction seen as a distinctive feature in every patient of CRPS, is of such severity that even considerable passive effort by a physiotherapist fails to mobilize these muscles to increase the ROM. Without USGDN, there prevails a yo-yo situation of minuscule improvement with physiotherapy followed by recurring restrictions of movement due to resistance by the abnormal muscle and pain which impede all such efforts at mobilization. Successive, incremental muscle relaxation and pain relief by USGDN allows better passive stretches to achieve coordinated movements. The active ROM follows more slowly because the patient has to regain the requisite power with strengthening exercises. Systematic alternate needling of the antagonist/ agonists followed by passive physiotherapy provided us with the ideal treatment to overcome the motor disability of CRPS with demonstrably improved ROM of 4-50 with each USGDN session. Needling the antagonists and agonists specific to any remaining restriction restored the ROM. This needling technique is based on anatomy of muscles around the joints, physiology of muscle contraction/relaxation and dynamics of movement. Utilizing it for the first time in CRPS, we found that USGDN is the much-needed ideal tool to optimize the effects of Physiotherapy.
This understanding of CRPS inflammatory process has increased my respect for physiotherapists tremendously because hitherto they were managing to produce some improvement in CRPS patients even though it was a tightrope walk for both the patients and physiotherapists. Less movements mean more stiffness, deterioration and no improvement, and little more exercises and the patient deteriorates with exacerbations of inflammation. This exacerbation is double edged in that not only is there inflammation around the hand tendons but also an increase in stiffness of muscles and worsening co-contraction. It was a testament to their dedication, patience and perseverance as well as the determination and endurance of CRPS patients that historically physiotherapy has been the consistent mainstay of CRPS treatment. Unfortunately, there appears to be little uniformity amongst physiotherapy techniques utilized for CRPS. (77) ‘Physiotherapy’ appears to be an umbrella term to be interpreted as mobilization exercises of various kinds according to the knowledge of CRPS or lack thereof of the physiotherapist.
USGDN, by reducing the co-contraction reduces both the problems of taut muscles and the consequent tenosynovial friction/inflammation and actually makes physiotherapy much easier. Any exacerbation of co-contraction by an intensive but productive session of physiotherapy can be reversed by the very next session of USGDN which invariable reduces the tenosynovitis symptoms. This predictable relief of pain makes the patients gain the confidence to work with the physiotherapist making graded reduction of co-contraction accompanied by return of normal coordination and disability improvement an achievable goal. It has been our routine observation that,
- The most significant benefit of USGDN to the patient is the reduction of both rest and movement pains with restoration of sleep disturbances within 2-3 sessions of USGDN. Once pain and stiffness relief is achieved, these symptoms do not recur at the original intensity even after intense physiotherapy.
- Next are the sensory symptoms like numbness, hypersensitivity, allodynia (normal touch of clothes, breeze perceived as pain) insect crawling sensations, shocks etc are reduced with each session and relieved within 3- 4 sessions. Once relief is achieved these symptoms do not recur. There are very fine muscle fibres (dermal motor elements) in the skin and erector pili muscles which cause goosebumps on exposure to cold. These muscle elements in the skin go into spasm in CRPS and are involved in the causation of sensory manifestations of CRPS. When needles are introduced through the skin to reach to the deeper muscles, they relieve the spasm of these dermal muscles.
- The warmth of CRPS limb is invariably reduced by USGDN as documented by skin temperature readings before and after a session. This is one of the most obvious and consistent findings in all CRPS patients. (figure 18) Warmth as a symptom does recur after intensive physiotherapy but subsides after the next USGDN. After about 5-7 sessions the recurrence of warmth does not occur.
- The sudomotor symptom of swelling takes about 7-14 to disappear completely. Initially swelling takes 1-2 days to reduce after USGDN. The patients present the next day with an obvious reduction of swelling. However excessive use of the hand, or intense physiotherapy can cause a recurrence of swelling and warmth in the first fortnight, but this is usually relieved by next session. We routinely observe that the initial tenosynovial effusion in the hands disappears for good after 10-15 days and does not recur thereafter.
- The color changes take about a 1-2weeks to normalize and do not recur thereafter.
- The motor improvement keeps happening with each USGDN session all along the treatment period of 20-40 days. It is the motor symptoms that take the longest to recover. The dystonia is replaced by purposeful movements, the range of motion improves at various joints by a few degrees as measured by goniometer after each session of USGDN. Since the whole limb and the neck are addressed at every session of USGDN, major changes are seen after each session at several joints, at the wrist, at the proximal middle and distal interphalangeal joints, supination and extension at elbow and all the movements at shoulder.
Once we understood that the clinical diagnostic criteria (Budapest criteria) of CRPS were actually manifestations of tenosynovitis (synovium of tendon) the mechanism of action of USGDN in specifically targeting the pathophysiology of CRPS became clear. It is actually the most specific treatment for CRPS, more than medications, sympathetic ganglion blocks, or CBPB or spinal cord stimulator which is a presently recommended treatment.
SCS modulates the pain sensation but does nothing to the muscle, hence these patients may get some pain relief which has been described in one review thus “up to 60% improvement in pain in 60% of patients 60% of the time”. (35-37)
Figure 18 – Temperature changes with USGDN
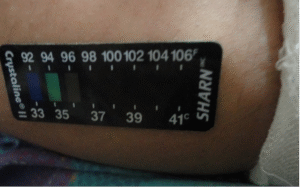
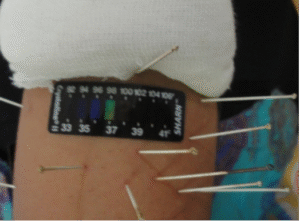
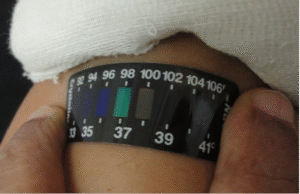
Temperature measured with a skin thermometer shows 37-380 centigrade before USGDN, 370 C with needles in situ and 350 C within 30 minutes after needle removal. These findings are uniformly observed in all patients. Clinically, patients report a reduction of warmth and a sense of coolness in the hand post USGDN, and also report a sensation of relaxation and easier movement after needle removal
Figure 19- Color changes in CRPS and their reversal by USGDN


Figure 19-This patient with CRPS of right hand with a dark skin and swelling over the little and ring fingers which became normal after treatment.
In our practice USGDN has become the sole therapy which produces 100% relief of rest pain within the first week and movements pains after 30-45 days of treatment AND 90-100% relief of disability at the completion of treatment. CBPB which we started out with, has become a secondary treatment being more of a complementary therapy reserved for specific indications like
- Patients who have a fear of needles,
- Patients in extremely severe pain who just cannot think of having needles inserted into them.
- Patients with severe dystonic movements where needles provoke an initial worsening of movements before the later quiescence. The co-contraction locks the agonist and antagonist muscles in severe cramps. In these patients the pain relief from CBPB becomes very useful for the first few sessions of USGDN.
- Patients who have come with a short time frame for treatment usually from other countries or other parts of India.
Hitherto out of a total 220 CRPS reversals, our first 8 patients had only CBPB and physiotherapy, 40 patients received combination of CBPB, USGDN and physiotherapy and 119 patients received only USGDN for Upper extremity CRPS. We have also successfully reversed lower extremity CRPS in 53 patients with involvement of ankle, knee and hip. For lower extremity CRPS, 32 out of 53 patients received a combination of USGDN, physiotherapy and a complementary neural interventions like continuous sciatic block, Lumbar plexus block and pulsed radiofrequency of entire innervation of knee and 21 patients received only USGDN. Thus 119 patients of Upper extremity CRPS and 21 patients of lower extremity CRPS have had successful reversal of CRPS with USGDN as the sole treatment modality at Ashirvad.
A striking feature of our CRPS reversal is an unequivocal pain relief within the first 10 days and gradual but ongoing disability relief over the next 3-6 weeks. We believe that this success is because of a paradigm shift in our understanding of CRPS; that the central pathology of CRPS is an abnormal co-contraction of the agonist /antagonist muscles of movements. Movements of the severely co-contracted muscles lead to secondary digital Teno synovial friction and inflammatory tendinosis in the hand, or ankle or knee. It is this Teno synovial inflammation which gives rise to pain, sensory, sudomotor and vasomotor manifestations which form the Budapest criteria of CRPS.
The abnormal co-contraction of CRPS affected muscles responds with exquisite sensitivity to ultrasound guided dry needling (USGDN) which accurately targets the co-contracted agonist/antagonist muscle combinations to relax them and restore their normal co-ordinated function. This automatically reduces the synovial friction and resolves the inflammatory tendinoses in the hand, or ankle or knee thereby reversing the pain, vasomotor, sudomotor and sensory features. Furthermore, the post needling muscle relaxation reduces the stiffness, weakness and dystonia with restoration of normal coordinated movements with dramatic improvement of disability.
Musculoskeletal ultrasonography (MSKUSG) has been of immense importance in corroborating our hypothesis by demonstrating the primacy of muscle pathology in CRPS. The disruption of muscle sonoanatomy in CRPS affected muscles is objective evidence that is uniformly demonstrable with ultrasonography, and we have described the importance of MSKUSG as a diagnostic investigation in upper extremity CRPS (51) and is very useful in distinguishing neuropathic pain from CRPS. (52) We have also described the restoration of the initial muscle structure disruption and motor function recovery that occurs after USGDN. (53)
To summarize, CRPS remains an unsolvable enigma in pain clinics of the world because the importance of muscle pathology has not been explored. At Ashirvad we have focussed on this problem to get an unequivocal and predicatble resolution of not just pain but also the disability associated with CRPS
References
- Merskey H, Bogduk N. Classification of Chronic Pain.IASP Task Force on Taxonomy. Seattle: IASP Press; 2nd 1994.
- Harden NR, Bruehl S, Perez RSGM, et al. Validation of proposed diagnostic criteria (the “Budapest Criteria”) for Complex Regional Pain Syndrome. Pain. 2010; 150:268-274
- Ferraro MC, O’Connell NE, Sommer C, Goebel A, Bultitude JH, Cashin AG, Moseley GL, McAuley JH. Complex regional pain syndrome: advances in epidemiology, pathophysiology, diagnosis, and treatment. The Lancet Neurology. 2024 May 1;23(5):522-33.
- Zalewski A, Andreieva I, Wiśniowska J, Tarnacka B, Gromadzka G. Clinical and Molecular Barriers to Understanding the Pathogenesis, Diagnosis, and Treatment of Complex Regional Pain Syndrome (CRPS). International Journal of Molecular Sciences. 2025 Mar 11;26(6):2514.
- Harden R. N, Baron R, Jänig W. Complex Regional Pain Syndrome IASP Press Seattle, 2001. 338 pages. ISBN 0-931092-41-8
- Harden RN, Bruehl S, Stanton-Hicks M, Wilson PR. Proposed new diagnostic criteria for CRPS. Pain Med. 2007; 8:326–331.
- Roberts WJ A hypothesis on the physiological basis of causalgia and related pains Pain 1986;24 297-311.
- Campbell JN, Meyer RA, Raja SN. The painful sequelae of nerve injury. Jänig W, Baron R. Complex regional pain syndrome is a disease of the central nervous system. Clin Auton Res.2002 ; 12(3): 150-64.
- Birklein F, Drummond PD, Wenwu Li, et al. Activation of cutaneous immune responses in complex regional pain syndrome. J Pain. 2014; 15:485-95
- Oaklander AL, Fields HL. Is reflex sympathetic dystrophy/complex regional pain syndrome type I a small‐fiber neuropathy? Annals of Neurology 2009 ;65 (6) :629–638.
- Eisenberg E, Chistyakov AV, Yudashkin M, Kaplan B,Hafner H, Feinsod M: Evidence for cortical hyperexcitability of the affected limb representation area in CRPS: A psychophysical and transcranial magnetic stimulation study. Pain 2005; 115:219 –20
- Vaneker M, Wilder-Smith OH, Schrombges P, de Man-Hermsen I, Oerlemans HM: Patients initially diagnosed as “warm” or “cold” CRPS 1 show differences in central sensory processing some eight years after diagnosis: A quantitative sensory testing study. Pain 2005; 115:204–11
- Alexander GM, van Rijn MA, van Hilten JJ, Perreault MJ, Schwartzman RJ: Changes in cerebrospinal fluid levels of pro-inflammatory cytokines in CRPS. Pain 2005;116:213–9
- Prasad, MD A, Chakravarthy, MD K. Review of complex regional pain syndrome and the role of the neuroimmune axis. Molecular Pain. 2021 Mar;17:17448069211006617.
- Stanton-Hicks M, Burton A, Carr D, et al. An updated interdisciplinary clinical path way for CRPS: report of an expert panel. Pain Practice 2002; 2:1-16.
- Jung YH, Kim H, Jeon SY, Kwon JM, Lee WJ, Kim YC, Jang JH, Choi SH, Lee JY, Kang DH. Brain metabolites and peripheral biomarkers associated with neuroinflammation in complex regional pain syndrome using [11C] -(R)-PK11195 positron emission tomography and magnetic resonance spectroscopy: a pilot study. Pain Medicine. 2019 Mar 1;20(3):504-14.
- Knudsen LF, Terkelsen AJ, Drummond PD, Birklein F. Complex regional pain syndrome: a focus on the autonomic nervous system. Clinical Autonomic Research. 2019 Aug 1; 29:457-67.
- Lee HJ, Lee KH, Moon JY, Kim YC. Prevalence of autonomic nervous system dysfunction in complex regional pain syndrome. Regional Anesthesia & Pain Medicine. 2021 Mar 1;46(3):196-202.
- Juottonen K, Gockel M, Sile´n T, Hurri H, Hari R, Forss N: Altered central sensorimotor processing in patients with complex regional pain syndrome. Pain 2002; 98:315–23
- Trojan J, Speck V, Kleinböhl D, Benrath J, Flor H, Maihöfner C. Altered tactile localization and spatiotemporal integration in complex regional pain syndrome patients. European Journal of Pain. 2019 Mar;23(3):472-82.
- Lewis JS, Newport R, Taylor G, Smith M, McCabe CS. Visual illusions modulate body perception disturbance and pain in Complex Regional Pain Syndrome: A randomized trial. European Journal of Pain. 2021 Aug;25(7):1551-63.
- Ten Brink AF, Halicka M, Vittersø AD, Keogh E, Bultitude JH. Ignoring space around a painful limb? No evidence for a body-related visuospatial attention bias in complex regional pain syndrome. cortex. 2021 Mar 1;136:89-108.
- Lebel A, Becerra L, Wallin D, Moulton EA, Morris S, Pendse G, Jasciewicz J, Stein M, Aiello-Lammens M, Grant E, Berde C, Borsook D: fMRI reveals distinct CNS processing during symptomatic and recovered complex regional pain syndrome in children. Brain 2008; 131:1854 –79
- Pohóczky K, Kun J, Szentes N, Aczél T, Urbán P, Gyenesei A, Szőke É, Sensi S, Dénes Á, Goebel A, Tékus V. discovery of novel targets in a complex regional pain syndrome mouse model by transcriptomics: TNF and JAK-STAT pathways. Pharmacological research. 2022 Jul 9:106347.
- Pohóczky K, Kun J, Szentes N, Aczél T, Urbán P, Gyenesei A, Szőke É, Sensi S, Dénes Á, Goebel A, Tékus V. discovery of novel targets in a complex regional pain syndrome mouse model by transcriptomics: TNF and JAK-STAT pathways. Pharmacological research. 2022 Jul 9:106347.
- de Rooij AM, Florencia Gosso M, Haasnoot GW, Marinus J, Verduijn W, Claas FH, van den Maagdenberg AM, van Hilten JJ: HLA-B62 and HLA-DQ8 are associated with Complex Regional Pain Syndrome with fixed dystonia. Pain 2009; 145:82–5
- Bruehl S: Do psychological factors play a role in the onset and maintenance of CRPS?, Complex Regional Pain Syndrome.Edited by Harden RN, Baron R, Janig W. Seattle, IASP Press, 2001
- Bruehl S, Harden RN, Galer BS, Saltz S, Backonja M, Stanton-Hicks M. Complex regional pain syndrome: are there distinct subtypes and sequential stages of the syndrome? Pain2002; 95(1-2): 119-24.
- Bonica JJ: Causalgia and other reflex sympathetic dystrophies, Management of Pain, 2nd edition. Edited by Bonica
- Schürmann M, Zaspel J, Löhr P et al. Imaging in early posttraumatic complex regional pain syndrome: a comparison of diagnostic methods. Clin J Pain2007; 23(5): 449-57.
- Harden RN, McCabe CS, Goebel A, Massey M, Suvar T, Grieve S, Bruehl S. Complex Regional Pain Syndrome: Practical Diagnostic and Treatment Guidelines. Pain Medicine. 2022 May;23(Supplement_1):S1-53.
- Raja SN, Buvanendran A, Marcondes L. Complex Regional Pain Syndrome: A Comprehensive Qualitative Research Study on Unmet Needs in the “Patient Journey”. Journal of Pain Research. 2021;14:2391.
- Mangnus TJ, Bharwani KD, Dirckx M, Huygen FJ. From a Symptom-Based to a Mechanism-Based Pharmacotherapeutic Treatment in Complex Regional Pain Syndrome. Drugs. 2022 Mar 5:1-21.
- Javed S, Abdi S. Use of anticonvulsants and antidepressants for treatment of complex regional pain syndrome: a literature review. Pain Management. 2021 Mar;11(2):189-99.
- Chmiela MA, Hendrickson M, Hale J, Liang C, Telefus P, Sagir A, Stanton-Hicks M. Direct peripheral nerve stimulation for the treatment of complex regional pain syndrome: a 30-year review. Neuromodulation: Technology at the Neural Interface. 2021 Aug 1;24(6):971-82.
- Bruehl S. Complex regional pain syndrome. BMJ. 2015 Jul 29;351.
- Pinckard-Dover H, Palmer A, Petersen EA. A review of neuromodulation for treatment of complex regional pain syndrome in pediatric patients and novel use of dorsal root ganglion stimulation in an adolescent patient with 30-month follow-up. Neuromodulation: Technology at the Neural Interface. 2021 Jun 1;24(4):634-8.
- Smart KM, Ferraro MC, Wand BM, O’Connell NE. Physiotherapy for pain and disability in adults with complex regional pain syndrome (CRPS) types I and II. Cochrane Database of Systematic Reviews. 2022(5).
- Wie C, Gupta R, Maloney J, Pew S, Freeman J, Strand N. Interventional modalities to treat complex regional pain syndrome. Current Pain and Headache Reports. 2021 Feb;25(2):1-6.
- Zacharias NA, Karri J, Garcia C, Lachman LK, Abd-Elsayed A. Interventional radiofrequency treatment for the sympathetic nervous system: a review article. Pain and Therapy. 2021 Jun;10(1):115-41.
- Zhao J, Wang Y, Wang D. The effect of ketamine infusion in the treatment of complex regional pain syndrome: a systemic review and meta-analysis. Current pain and headache reports. 2018 Feb;22(2):1-8.
- Xu J, Herndon C, Anderson S, Getson P, Foorsov V, Intravenous Ketamine Infusion for Complex Regional Pain Syndrome: Survey, Consensus, and a Reference Protocol Pain Medicine, Volume 20, Issue 2, 2019, Pages 323–334
- Ho E, Yazdanpanah N, Johnson H, Drukman B, Chang A, Agarwal S. Parameters of spinal cord stimulation in complex regional pain syndrome: systematic review and meta-analysis of randomized controlled trials. Pain Physician. 2022;25(8):521.
- Hoikkanen T, Nissen M, Ikäheimo TM, Jyrkkänen HK, Huttunen J, von und zu Fraunberg M. Long-Term outcome of spinal cord stimulation in complex regional pain syndrome. Neurosurgery. 2021 Oct;89(4):597.
- Mohabbati V, Mohabbati P, Papan M. A review of waveform and paradigm variations of spinal cord stimulation for the treatment of complex regional pain syndrome. Journal of Pain Research and Management. 2025 Feb 20;1(1):43-56.
- Eriksen LE, Terkelsen AJ, Blichfeldt‐Eckhardt MR, Sørensen JC, Meier K. Spinal cord stimulation in severe cases of complex regional pain syndrome: A retrospective cohort study with long‐term follow‐up. European Journal of Pain. 2021 Nov;25(10):2212-25.
- Frederico TN, da Silva Freitas T. Peripheral nerve stimulation of the brachial plexus for chronic refractory CRPS pain of the upper limb: description of a new technique and case series. Pain Medicine. 2020 Aug 1;21(Supplement_1):S18-26
- Żyluk A, Puchalski P. Effectiveness of CRPS treatment: A systematic review. Neurologia i neurochirurgia polska. 2018 Mar 12.
- Vas LRetrospective Review of Successful and Complete Reversal of Complex Regional Pain Syndrome and the Associated Disability of Upper and Lower Extremities in 205 Consecutive Patients IASP Poster selected for video presentation in the virtual IASP conference 2020.
- Vas L, Pai R. Complex regional pain syndrome‐type 1 presenting as deQuervain’s stenosing tenosynovitis. Pain Physician 2016;19:E227‐34.
- Vas LC, Pai R, Radhakrishnan M. Ultrasound appearance of forearm muscles in 18 patients with complex regional pain syndrome 1 of the upper extremity. Pain Pract 2013;13:76‐88.
- Vas LC, Pai R. Musculoskeletal ultrasonography to distinguish muscle changes in complex regional pain syndrome type 1 from those of neuropathic pain: An observational study. Pain Pract 2016;16:E1‐13.
- Vas LC, Pai R, Pattnaik M. Musculoskeletal Ultrasonography in CRPS: Assessment of Muscles Before and After Motor Function Recovery with Dry Needling as the Sole Treatment. Pain physician2016; 19: E163-80
- Vas L, Pai R. Successful Reversal of Complex Regional Pain Syndrome Type 1 of Both Upper Extremities in Five Patients. Letter, Pain Medicine2012; 13: 1253-6.
- Vas L and Pai R. Reversal of complex regional pain syndrome type 2 and the subsequent management of complex regional pain syndrome type 1 occurring after corrective surgery for residual ulnar claw.Pain Medicine 2014; 15: 1059-1063.
- Vas L, Pai R, Geete D, Verma CV. Improvement in CRPS after deep dry needling suggests a role in myofascial pain. Pain Med 2018;19:208‐12.
- Vas L. Commentary: Selective fiber degeneration in the peripheral nerve of a patient with severe complex regional pain syndrome. Front Neurosci 2019;13:19.
- R,Vas. L, Patnaik. M, Ultrasound guided intra-articular injection of radio-ulnar & radio-humeral joints; and dry needling of the affected limb muscles to relieve the fixed pronation deformity and secondary myofascial issues in a case of Complex Regional Pain Syndrome- type 1 (CRPS-1) Pain Practice, 2018; 18 (2) 273–282
- Vas L.Effectiveness of Ultrasound guided Dry Needling in Chronic pain Pain News 2019 ,17;4:202-212
- Vas LC. Ultrasound guided dry needling: Relevance in chronic pain. Editorial J Postgrad Med 2022;68:1-9.
- Eisenberg E, Geller R, Brill S. Pharmacotherapy options for complex regional pain syndrome. Expert Rev Neurother. 2007 May; 7(5): 521-31.
- Cepeda MS, Lau J, Carr DB. Defining the therapeutic role of local anesthetic sympathetic blockade in complex regional pain syndrome: a narrative systematic review. Clin J Pain 2002; 18:216–233-40
- Nelson DV, Stacey BR Interventional therapies in the management of complex regional pain syndrome. Clin J Pain. 2006 Jun; 22(5): 438-42.
- Cepeda MS, Carr DB, Lau J. Local anesthetic sympathetic blockade for complex regional pain syndrome. Cochrane Database Syst Rev. 2005 Oct 19;(4): CD004598.
- Ribbers G, Geurts A, Rijken R et al. Axil lary brachial plexus blockade for the reflex sympathetic dystrophy syndrome. Int J Re habil Res 1997; 20:371-380.
- Murray P, Atkinson R. Continuous axillary brachial plexus blockade for reflex sympa thetic dystrophy. Anaesthesia 1995; 50:633-635.
- Wang L, Chen H, Chang P et al. Axillary bra chial plexus block with patient-controlled analgesia for complex regional pain syn drome type I: A case report. Reg Anesth Pain Med 2001; 26:68-71.
- Day M, Pasupuleti R, Jacobs S. Infraclavicular Brachial Plexus Block and Infusion for Treatment of Long-Standing Complex Regional Syndrome Type 1: A Case Report.Pain Physician. 2004; 7:265-268,
- Dadure C, Motais F, Ricard C, Raux O, Troncin R, Capdevila X.Continuous peripheral nerve blocks at home for treatment of recurrent complex regional pain syndrome I in children. 2005 Feb; 102(2): 387-91.
- Mosby’s Medical Dictionary. 8th edition. Elsevier, St Louis, 2009.
- Adams MA, Black SM, Dolan P, Partridge. Functional anatomy of the musculoskeletal system. In: Standring S (ed). Gray’s Anatomy. 40th edition. Churchill Livingstone, Philadelphia, 2008, pp 114-115.
- Agur AMR, Dalley AF (eds). Grant’s Atlas of Anatomy. 11th edition. Lippincott Wil- liams & Wilkins, Philadelphia, 2009, pp 541.
- Jankovic J, VanDer Linder C. Dystonia and tremor induced by peripheral trauma: predisposing factors. J Neurol Neu- rosurg Psychiatry 1998; 51:1512-1519.
- Hudak PL, Amadio PC, Bombardier C. Development of an upper extremity out- come measure: the DASH (disabilities of the arm, shoulder and hand) [cor- rected]. The Upper Extremity Collabora- tive Group (UECG). Am J Ind Med 1996; 29:602-608. Erratum in: Am J Ind Med 1996; 30: 372.
- Vas L, Pai R, Khandagale N, et al. Myofascial Trigger Points as a Cause of Abnormal Co-contraction in Writer’s Cramp. Pain Med. 2015;16(10):2041-2045.
- Harden RN, Bruehl SP. Diagnosis of complex regional pain syndrome: Signs, symptoms, and new empirically derived diagnostic criteria. Clin J Pain 2006;22(5):415–9.
- DalyAE,BialocerkowskiAE.Does evidence support physiotherapy management of adult complex regional pain syndrome type one? A systematic review. Euro Jour Pain 2009; 13:339-353.



