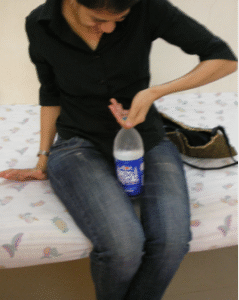
This is a pain condition that occurs after any injury, surgery, excessive use with overactivity (repetitive strain injury syndromes) and occasionally may occur spontaneously. It may involve any part of the body, but the upper limb is most commonly involved (figure 1) followed by lower limb (after knee or ankle/foot surgery or injury) It may rarely involve both upper or both lower limbs simultaneously. Spreading CRPS from one limb to the other has also been described. Less commonly, this may also occur in face after head neck surgery, and in chest or abdomen after surgery on these areas. CRPS has been our special interest at Ashirvad because we have developed a de novo innovative treatment which has been extremely successful in reversing this difficult condition in a large number of patients. However, in world literature it has been described as a difficult condition to treat and has been a nemesis in all the pain clinics across the world. In this blog I give a brief presentation of the world view initially and then proceed to give details of our successful experience with CRPS
| Upper limb surgery | N | CRPS | Lower limb surgery | N | CRPS |
| Open reposition distal radius | 6,581 | 77 (1.17% | Arthrodesis ankle joint open | 412 | 4 (0.97%) |
| Hand resection arthroplasty | 566 | 6 (1.06%) | Arthroscopy ankle joint operation | 513 | 4 (0.78%) |
| Hand tendon, ligament, fascia repair | 2573 | 21 (0.82%) | Open reposition distal fibula & tibia | 4543 | 27 (0.59% ) |
| Partial Shoulder replacement | 129 | 1 (0.78%) | Foot surgery | 3405 | 17 (0.50%) |
| Surgery on hand arm nerves | 930 | 7 (0.75%) | Knee joint replacement revision | 984 | 4 (0.41%) |
| Shoulder joint replacement | 1421 | 4 (0.28%) | Arthroscopy knee operation | 11,189 | 18 (0.16%) |
| Shoulder surgery | 8456 | 18 (0.21%) | Hip joint replacement revision | 1264 | 2 (0.16%) |
| Proximal humerus surgery | 2057 | 4 (0.19%) | Hip joint replacement | 19164 | 25 (0.13%) |
| Arthrodesis interphalangeal | 120 | 0(0.00%) | Toe amputation
Knee joint replacement revision. Removal material femur. |
1525
13846 913 |
2 (0.13%). 9 (0.07%) 1 (0.11%) |
| Total for upper-limb surgery | 22,833 | 138(0.60) | Total for lower-limb surgery | 57,758 | 113(0.20%) |
Table 1: CRPS Incidence after different types of surgery. K.Teichmu ̈lleretal.·9(2024)e1210 PAINReports
The International Association for the Study of Pain (IASP) has defined CRPS-1 as ‘‘a variety of painful conditions following injury which appears regionally, having a distal predominance of abnormal findings, exceeding in both magnitude and duration the expected clinical course of the inciting event often resulting in significant impairment of motor function and showing variable progression over time”. It has been called CRPS-2 when it occurs when an obvious nerve damage. can be demonstrated. IASP goes on to describe CRPS as a chronic, progressive disease characterized by severe pain, motor impairment, and “inflammation like” changes in the distal extremity. The CRPS limb is very painful, looks angry, red and is swollen as if there is some infection and inflammation (figure 1). Inflammatory mediators are found to be raised in the venous blood draining the CRPS limb. However, there is no infection because all the tests that suggest an infection like a raised white blood cell count, or pus collection are negative.
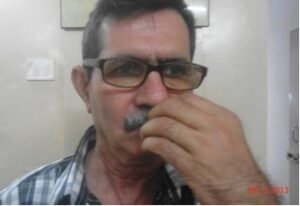
Figure 1: The typical appearance of CRPS limbs and face with color, temperature and size asymmetry









Figure 1: The left hand is swollen, hot, stiff and painful, the operated right knee looks much darker, warm and extremely stiff and painful, operated right ankle swollen, dark, painful and unable to bear weight . The last image shows a swollen dark and extremely painful face due to CRPS after cancer surgery.
2nd row : shows 2 images of CRPS-1 left leg, left hand. The third image shows the typical movement restriction at elbow where patient is unable to turn her palm upwards. Fourth image showsa patient with CRPS-2 with a median nerve injury causing loss of sensation in the first 3 fingers. While cooking she developed a burn injury with an ulcer in the index finger. The 5th image shows CRPS in both hands, an unusual presentation of bilateral CRPS.
IASP has defined certain symptoms and signs as Clinical diagnostic criteria to as a guide or basis to diagnose CRPS. A modification of these criteria called Budapest criteria have been proposed and are commonly used as essential criteria to diagnose CRPS. They are also used to assess response to CRPS treatments. (1, 2)
Two recent scientific reviews published in 2024 and 25 (3,4) state that despite many scientific advances, CRPS continues to present diagnostic and therapeutic challenges for clinicians because 1. Pathophysiological mechanisms are incompletely understood at present.
- The clinical presentation is heterogeneous, due to interaction of multiple systems.
- There is often poor response to treatment.
- Validated diagnostic criteria have lacked guidance to assess fluctuating and spreading symptoms. (5) There has been limited high-quality clinical guidance to manage the debilitating symptoms of CRPS, and their impact on the lives of those affected. CRPS is not only difficult to treat but also difficult to study. This is because the challenges with CRPS are
- The heterogeneity of the patient population,
- The influence of pain coping strategies and psychological factors,
- The impact of sociocultural factors.
Table -2: NEW IASP CLINICAL DIAGNOSTIC CRITERIA (BUDAPEST) FOR CRPS
- Continuing pain, which is disproportionate to any inciting event
- Must report at least one symptom in three of the four following categories:
- Sensory: reports of hyperesthesia and/or allodynia
- Vasomotor: reports of temperature asymmetry and/or skin color changes and/or skin color asymmetry
- Sudomotor/edema: reports of edema and/or sweating changes and/or sweating asymmetry
- Motor/trophic: reports of decreased ROM and/or motor dysfunction (weakness, tremor, dystonia) and/ or trophic changes (hair, nail, skin)
- Must display at least one sign at time of evaluation in two or more of the following categories:
- Sensory: evidence of hyperalgesia (to pinprick) and/or allodynia (to light touch and/or deep somatic pressure and/or joint movement)
- Vasomotor: evidence of temperature asymmetry and/ or skin color changes and/or asymmetry
- Sudomotor/edema: evidence of edema and/or sweat- ing changes and/or sweating asymmetry
- Motor/trophic: evidence of decreased ROM and/or motor dysfunction (weakness, tremor, dystonia) and/ or trophic changes (hair, nail, skin)
- There is no other diagnosis that better explains the signs and symptoms
Adapted from Harden RN, Bruehl S, Stanton-Hicks M, Wilson PR. Proposed new diagnostic criteria for CRPS. Pain Med. 2007; 8:326–331.(6)
The pathophysiological mechanisms leading to CRPS have been discussed in numerous publications, all of which reiterate that the causes of CRPS are multifactorial involving,
- Both peripheral and central nervous system mechanisms (7-11).
- Peripheral and central sensitization (12,13),
- Neuroinflammation(14-17),
- Altered sympathetic and catecholaminergic function(7,18,19),
- Altered somatosensory representation in the brain(20-24),
- Genetic factors(25,26), and
- Psychophysiologic interactions(27)
- Confusions persist regarding different CRPS subtypes, and progression of symptoms through hypertrophic, dystrophic and atrophic stages, all of which present different symptoms (28,29)
- Diagnostic investigations (30), and treatments remain poorly defined. (3,4, 31- 48)
- The pain literature says that at the present time, there is no effective method of treatment of CRPS though a large number of treatments (pharmacologic treatment, nerve blocks, psychotherapy, and physiotherapy) have been investigated. Current treatments focus on achieving varying degrees of pain reduction rather than aim for disability reduction/relief.
All this emphasizes that CRPS has remained a major enigma and a nemesis amongst chronic pain conditions with marked symptoms of inflammation in its early phase, which disappear in its later stages, but its hallmark symptom of stiffness and pain persist all the time. CRPS pain exhibits features of neuropathy like burning, shocks, tingling, pulling pains numbness, paradoxical pain in an area perceived as being numb by the patient, and skin becomes very oversensitive and tender. However, the most dominant and striking symptom is the severe stiffness of limb associated with weakness where the patient just cannot do anything with that hand, like picking up objects or make a fist or perform any of the fine hand functions like writing, sewing or playing musical instruments. Even slight movements are extremely painful which makes the patient avoid movements. As they avoid movements the swelling and pain may reduce slightly but the stiffness increases. And the moment they try to resume some hand movements again; both the swelling and pain return with redoubled vigor. When the foot is involved, the foot movements and weight bearing become extremely painful with highly restricted foot and ankle movements.
As these descriptions show, CRPS is a perplexing clinical entity with not just pain and swelling but also major movement difficulties. Its cause, how or why the disease develops and progresses, what investigation can be performed to confirm the clinical diagnosis or even how to treat its various problems, currently remains undefined in world literature.
Ashirvad experience of CRPS: Our experience with CRPS has been in stark contrast to the world scenario. In the past 20 years we have seen routine reversal of consecutive CRPS patients with167 patients having upper extremity CRPS (both CRPS 1 and 2) and 53 patients with lower extremity CRPS (both 1 and 2) (49-60). By consecutive, we mean that out of 220 patients who opted to have the treatment, every patient showed improvement not just of pain but also disability.
Our treatment has evolved over the last 20 years. Our learning of CRPS happened in a very unusual manner; we achieved success first and then had to puzzle out just why we were achieving success at all! It started out with only nerve blocks, then over the years as we understood the importance of muscle pathology in CRPS pathophysiology, (disease process) it became a combination of nerve treatments along with a muscle treatment called ultrasound guided dry needling. (USGDN) Finally, as the primacy of muscle pathology became obvious, we came to understand that USGDN is the perfect antidote to the problems of CRPS and is a far more important treatment with extremely reliable results. This is diagonally opposite to the world understanding of CRPS as an enigma, a neural disorder, with a total lack of any acknowledgement of muscles as a causative factor.
The scientifical analysis that led us to arrive at our current understanding of CRPS as a primary muscle disorder happened in the years 2003-2005. After 2006, our success with every patient that we have treated in the last 20 years has reiterated our understanding that muscle disorder is of primary importance in CRPS. When we address the muscle disorder, not only is the pain of CRPS permanently reversed but more importantly the disability also gets reversed. As such we use only USGDN as the primary treatment, keeping the neural interventions like Stellate block and/or brachial plexus nerve blocks only for select patients with severe pains.
The evolution: Initially when we started treating CRPS in 2003 and 2004, the information at that time in the vast literature on CRPS including major textbooks on pain, was less than helpful, highly confusing, with many unproven hypotheses about what might cause it or how and why it manifests as it does. Unfortunately, none of the treatments developed on the basis of these hypotheses appeared to be consistently useful (16). For CRPS hand, the recommended treatment at that time was medications(61) and stellate ganglion block (SGB). Stellate ganglion provides the sympathetic nerve supply to the upper limb blood vessels to control the blood supply to the limb by either contracting or relaxing them. The exact mechanism of how a sympathetic block helps to relieve the pain in CRPS was not known and just who would benefit was also unpredictable. The literature was equally divided as to whether this might or might not be useful and many scientific reviews on the topic opined that there is no conclusive evidence to support these blocks. (62-64) If the block works, then these patients are considered to have sympathetically maintained pain which was relieved by the block and are given repeat blocks as and when needed, for future management (7). The patients in whom sympathetic blocks don’t relieve pain are considered to have a pain that is independent of sympathetic nerves and sympathetic blocks are not an option for future management (8).
In this scenario, I was not convinced that I should assume that my patients would have sympathetically maintained pain and that just a stellate ganglion block would suffice to relieve the pain in them. I was also dubious that even it was effective, a single injection of stellate ganglion could make a lasting difference to my patients, because sooner or later, the effect of SGB would wane and then what? While being an observer in pain clinics abroad I had seen many patients with recurrent CRPS pains coming for their 6 monthly dose of stellate blocks. But I did not want my patients to be indefinitely dependent on such a temporarily effective treatment. So, I decided to provide a more certain and lasting way to keep the pain relieved. In addition to the Stellate block which would block only the sympathetic nerve fibers, I decided to do a continuous block of the brachial plexus of nerves (CBPB) that supply both sensory and motor needs of the whole of upper extremity. The logic behind this decision was that CBPB would keep the whole limb continuously pain free for as long as it was maintained. The continuous suppression of hand pains by CBPB would help in ‘unwinding’ the ‘wind up’ of spinal sensitization as well as allow good physical therapy which would achieve the goal of relieving pain and the impairment of movement due to pain. I hoped that once the pain was completely suppressed it would not return so quickly. There were a few publications on CBPB for very short durations( up to 48 hours) (65-69) but Continuous ongoing somatic block made a more scientific sense to me rather than temporarily blocking only the sympathetic nerves. After a detailed discussion of the risk and benefits of CBPB, my initial 2 patients wanted to go ahead with the treatment. The results were very rewarding in that they both had about 50% pain relief after stellate block but after CBPB, both had complete and instantaneous relief of pain and distress. Thereafter, their sleep disturbances were relieved as well, and they started eating well and regained their interest in life. (figure 2)
Figure 2: Our first 2 CRPS patients, the lady with shoulder hand syndrome and the man with Colle’s fracture of wrist






Figure 2: The lady in first row presented with severe pain, sleep disturbances and inability to lift her right hand. Immediately after stellate ganglion block, she is obviously happy, but after combination therapy with continuous brachial plexus block (CBPB) + aggressive physiotherapy she is able to do her daily activities without pain. The man presented with severe pain in the swollen hot, left hand. The middle image shows the CBPB catheter under the dressings on chest connected to the elastomeric pump (the round object in his pocket). In both the patients despite the pain relief after CBPB, the patients could not make a fist or approximate their thumb to the fingertips making hand function very difficult. They could not even eat with their hands or write. Their hands simply did not have the strength to grasp doorknobs or other objects. Their motor improvement took a lot of determined effort where the physiotherapist had to coax and cajole them every day for a long time of 6-8 weeks.
Despite our success with pain relief, we were facing major problems with the motor impairment of CRPS where disability persisted despite the continuous nerve block. Perplexingly, the difficulties of hand movement persisted even though the limb was totally pain free making it obvious that in CRPS, pain and muscle stiffness were separate entities. The most notable thing in all these patients in 2004-2005 was that, though all pain was completely cut off by the CBPB, the movement difficulty persisted. The muscle stiffness still impeded their hand movement, and they could not do anything with their hands. The patients struggled to bend their fingers but were unable to make a fist. Being able to bring the fingers to the palm to make a fist is essential for practically every hand function. CBPB allowed the patients to work enthusiastically with the physiotherapist, but they had to work hard for every mm of movement of the fingers and hand that they regained.
Around this time, we were seeing women with breast cancer surgery, radiation and chemotherapy who had developed swollen upper limbs. We observed that these women also benefitted from CBPB and stellate ganglion blocks. Similar results were observed even in patients with CRPS of face.
Figure 3: patients with cancer who had CRPS of face after head neck and breast surgery.






Reduction of swelling and pain in the face and upper limb after steroid injection into the sympathetic ganglion that provides sympathetic nerve supply to face, and upper limbs called stellate ganglion
These results indicated that CRPS was not confined to limb injuries but could occur after cancer surgery as well. There were many cancer patients with various forms of CRPS whose pains were sympathetically maintained. In simple words this means that their sympathetic nerves were irritable and were causing a major part of the pain after breast and head neck surgeries and they could benefit from SGB.
The stiffness and weakness associated with inability to use the hand (Motor impairment of CRPS) continued to be a recurrent theme in my subsequent patients. CBPB would make them comfortable, but they continued to struggle with their stiffness and weakness which impeded purposeful movements of fingers and hand. Even passive movements where the physiotherapist was trying to bend their extremely stiff fingers to make a fist were not possible. This was because the fingers would simply not bend even when considerable pressure was applied and the patients would get pain despite the CBPB. When they returned the next day, their hand would show a complete recurrence of CRPS symptoms of hand looking angry swollen and red, but fortunately, the pain was not very prominent probably because of the CBPB. But if they did cryotherapy( dipping them in cold water) and rested the hand without physiotherapy for a day or two the symptoms would go down and then they could resume physiotherapy. Thus, physiotherapy acted like a double-edged sword causing a yo-yo of symptoms. The saving grace was the pain relief from CBPB where the patient continued to be comfortable in spite of a swollen hand, so they continued with the physiotherapy. For the physiotherapists also this was a novel experience because they had never worked with a patient of CRPS who was rendered pain free by a CBPB. Over time, both the physiotherapist and the patient appeared to grasp just how much the hand could be pushed, usually indicated by the patient’s pain that overrode the baseline relief from CBPB. This was usually about a 3-40 increase of ROM at each joint per session. However, once the physiotherapist achieved a better range of passive movement, the patients could follow with active movements within this increased pain free range of movement. This was a slow and painstaking process, but both the physiotherapist and the patients were positively motivated by the pain relief and comfort provided by CBPB. So, with each subsequent patient it was a reiteration of my original finding that it was not the pain that made movements difficult but the motor impairment which appeared to be an independent issue by itself unrelated to pain. I was also more and more convinced that the motor impairment that causes the stiffness of CRPS was a more crucial aspect of CRPS than the pain because once the patients regained hand function, pain was not an issue anymore and the CBPB could be discontinued. The difficulty in movement appeared to be because something was intrinsically wrong with the CRPS muscle. I realized that blocking the nerves was an indirect, roundabout way to address an intrinsic muscle stiffness, but I continued using CBPB because it seemed to be working. I was not sure about what I could do to improve this stiffness. The local anesthetic infusion from the CBPB made the hand completely pain free and provided the time for physiotherapy to work so the patients could gradually increase the range of motion at the joints of the fingers to make a fist. All my patients assured me that they were ready to accept the continued risk of infection as they had no intension of letting go of the CBPB which had made them so comfortable. So, the catheters were retained for 45 and 60 days in my initial 8 patient after which they were removed uneventfully. However, this is a potentially risky situation because a foreign body like the nerve catheter inside the body can predispose to serious infections. In our initial patients, I had planned to remove the CBPB after 1 week because longer we keep a foreign body like a nerve block catheter in situ, higher the risk of infection.
So, I started looking for treatments that could address the muscle stiffness of CRPS. By this time, I was already using Dry needling in various pain conditions with notable success. I had not used it in CRPS because I was still under the influence of the extensive (but unhelpful!) literature on CRPS which where the world authorities on CRPS firmly asserted that it was a nervous system disease. However, I got the opportunity to test my hypothesis that CRPS had an intrinsic muscle involvement in my next patient, young lady with spontaneous shoulder hand syndrome, one of the simpler forms of CRPS (fig 4). She had travelled from East Africa for her treatment in early 2006. Use of USGDN in her for the first time revolutionized our later treatment of CRPS.
Figure 4-The patient in whom dry needling was used for CRPS for the first time in 2006




Shoulder hand syndrome :swollen painful dark hand and painful restricted movements at left shoulder .
She responded very well to CBPB with relief of pain swelling at the hand and forearm and started sleeping well (Fig 5). She was very happy with her improvement but was rather miffed by my insistence that she should regain all the movements of the upper extremity. She still was unable to lift her arm at the shoulder because of a ‘catch’ as she described it, at 2 locations, one at the armpit and one at elbow. These were areas overlying the origin of a muscle called coracobrachialis at the coracoid process of scapula and insertion of the biceps muscle at the elbow. So, I decided to do DN of these muscles. The results after needle removal were so astonishing (figure 5) in that she had no pain in raising her hand all the way up.
Needless to say, the patient was thrilled with this improvement, and this improvement impressed me so much that I continued to do DN of her neck and whole upper limb for the next week.
The results of this DN were nothing short of miraculous. While my previous 7 patients had taken 45-60days of CBPB to get full range of movement, this lady achieved it in just 18days!
Fig 5- The patient with no rest pain after CBPB but abduction was still painful



Dry needling of the pectoralis major and minor and coracobrachialis at the anterior axillary fold of armpit and the biceps at the elbow immediately relieved her pain and she could raise her hand to full range
Figure 6 – The patient’s recovery after 18 days




At the end of 18 days the patient had a complete reversal of her CRPS regaining complete range of movements and had no pain at all. She remained in touch with us for 8 years and she remained normal.
I was not sure whether this was some kind of a fluke, or it was my lucky hunch paying off. Well, there was only one way of finding out and that was to repeat the same treatment in the next few patients of CRPS.
Figure 7- Patient seen 2013 with CRPS after internal fixation of wrist and humerus fractures




Patients with post-surgery CRPS unable to flex his fingers or make a fist and the left shoulder movements of abduction and internal rotation are painfully restricted.
Figure 8 The patient after 20 days of treatment


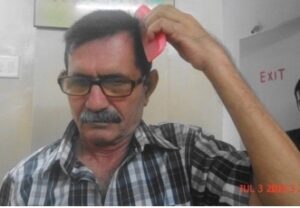
He is able to do delicate functions of hand like eating, holding a comb to comb his hair or the spectacle frame as well as those requiring strength like lifting a 1litre bottle of water. His shoulder has also improved to make overhead movements
I took the consent of patients after explaining to the patients that needling is a safe treatment so there was no risk involved other than few bruises which would disappear uneventful in a week or two. I repeated needling in my subsequent CRPS patients and good results kept coming in like clockwork (figures 7-9).
Figure 9 – The usual pattern of CRPS recovery at Ashirvad .

Figure 13- Patients present with a painful swollen hand and fingers in extended position unable to flex or make a fist. The pain is no longer a problem after 2-3 sessions of USGDN, and they start sleeping well. The movements also improve and by day 10-12 they are able to make a fist. As treatment proceeds, the patients improve steadily. By day 17 this patient is able to grasp the bulb of a dynamometer but is unable to squeeze it beyond 0 pounds / square inch. But by day 22 she is able to generate 4 pounds / square inch pressure which is adequate for most activities of daily life like turning doorknobs, fastening trousers etc
Addition of needling to other treatments of CRPS at that time like SGB and CBPB made a dramatic difference to our outcome reducing the time taken for complete recovery as well as the much-improved quality of recovery. Early on in our experience of USGDN with CBPB from 2006 to 2009, we used to take longer (5- 7weeks) to reverse CRPS, but over these years our USGDN techniques have been refined, and reversal is within 3-6 weeks so that CBPB could be cut down to 15-30 days by 2013 from 45-60 days that we used to take between 2004 to 2007.This was a great advantage because this reduced the risks of CBPB catheter complications like infection, accidental extrusion etc. In a few patients, even though there was accidental catheter extrusion at 12 and 15 days, the patients continued with their improvement with just DN.
The Initial dramatic efficacy of DN made us happy but we had no idea why or how it was working so well. No amount of mulling over this produced any answer. With the policy of not looking a gift horse in the mouth, we continued with USGDN till our 11th patient, a senior banker from Nigeria arrived for treatment. He had received knife injuries to his upper limb after which he just could not move his fingers. It was suspected that his tendons might have been cut, but the ultrasonologist opined that the tendons were intact. Fortunately for him he was referred to an experienced and discerning hand surgeon who suspected that post injury CRPS had made his hand completely useless and referred him to me. The CRPS was obvious on examination (figure 10) but interestingly, when I asked him to touch his fingertips to his thumb, he developed dystonia of the fingers without achieving any purposeful movement. As I watched his fingers twitching uncontrollably, it suddenly occurred to me that this was similar to the kind of trembling that comes on when we do something very strenuous with a lot of force struggling to hold a position using opposing muscle groups. The scientific name for this is agonist antagonist co-contraction.
Figure 10 Patient with knife injuries of left forearm and hand. When he tried to approximate the thumb to fingers he would develop severe dystonic tremors of left hand


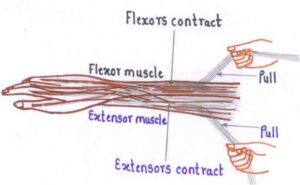

Figure 10– Note the narrowing of the left hand compared to the right hand. This narrowing which appears to be due to intense spasm of the interosseous muscles between the metacarpal bones. DN of these muscles reverses this narrowing and restores the palm to its normal size. When he attempted to touch the tip of his fingers to the thumb, he developed severe dystonic movements. We surmised that this was because of a simultaneous contraction of flexors and extensors called co-contraction.
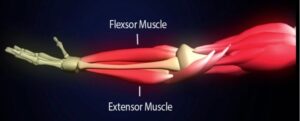
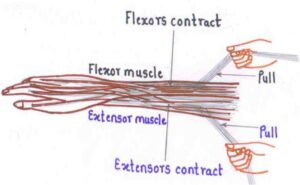
Physiologically, when a muscle that bends(flexes) the finger to the palm contracts, the muscles that pull the finger backwards away from the palm(extensors) should relax so that the flexor muscle bends the finger freely. Co-contraction is a mechanism where both groups of muscles, flexors(agonist) and extensors(antagonist) contract together simultaneously at the beginning of the movement and then the flexors muscles dominate the extensor muscles to achieve controlled flexion. (70-72) This is called “guiding” in mechanical engineering parlance. Normally this kind of co-contraction is a normal voluntary action that is performed at will, painlessly and easily to facilitate some complicated actions. For eg the wrist has to be fixed in slightly extended position so the fingers can bend repetitively to perform writing (fig 11).
The dystonic movements observed in this patient indicated that the co-contraction continued unabated even after the initiation of movement. This co-contraction observed in CRPS is abnormal in that it is highly exaggerated, present continuously in a resting hand even in absence of any attempts to move the fingers and is extremely painful. The patient has no control on it whatsoever.
Figure 11- physiological co-contraction
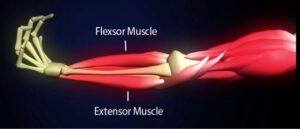
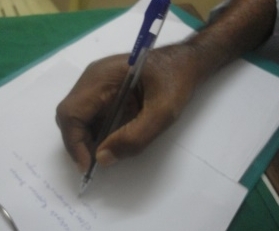
When digital flexors contract, extensors should relax and vice versa except when they contract together to act as fixators. eg wrist fixed in extension to optimize finger movement for writing. This co-contraction has a fixator function which is voluntary coming on at will, physiological and completely painless and can be terminated at will.
The abnormal co-contraction in CRPS induces a contradictory combination of weakness associated with stiffness (figure 12 13).
Figure 12- relief of co-contraction with USGDN


As a result of co-contraction, the same patient as in figure 11 is unable to grasp the bulb of the dynamometer before treatment but 17 days later after 7 sessions of USGDN he is able to passively approximate the fingers to palm
Any attempt to overcome it and perform a purposeful movement exaggerates it as seen in the dystonic movements in this patient. Treatment with USGDN under cover of CBPB relieved his dystonia within a week, and he went all the way to normalcy to return to Nigeria within a month. The surgery of course was not necessary, and this was a great benefit because any surgery in CRPS is likely to worsen CRPS.
Figure 13- Abnormal co-contraction of agonist and anatagonist muscles in CRPS



Co-contraction explained just why CRPS patients struggle so much to do any movement at all. It also explained the obviously dramatic success of USGDN which relaxes all the muscles in a graded systematic manner, actually reduces the co-contraction and finally replaces it with the delicate coordination required for normal movements. Jancovic etal have shown coactivation of agonist antagonist muscles in CRPS. (73) But I still had not worked out how or why co-contraction was connected to the inflammation of CRPS which is responsible for producing the clinical diagnostic criteria of IASP. As we saw more and more patients in the years 2006-9, we got more and more pieces of the CRPS jigsaw puzzle together but were still far away from making a coherent assembly to see the whole picture. We tried to publish our clinical data but found that these ideas were so out of box that no journal was ready to accept them. The logic of DN was obvious to us because we were seeing its success on a daily basis, but the reviewers who scrutinized our papers were people who had no experience with DN and most of them had probably never held a needle in their hands. As such they probably found it difficult to believe what we had written even though the pre and post treatment pictures told their own story (figure 14).
Most of our papers got rejected outright and there was not much we could do about it without some kind of objective evidence that could prove our hypotheses. This opportunity came in 2009. An ultrasonography (USG) machine company brought their machine for demonstration. So, I thought ‘let us see if the intrinsic muscle issues of CRPS can be visualized on USG’. I had two patients of CRPS in the clinic that day and what I saw on USG just blew me away. USG unequivocally showed in black and white what I had suspected all the time, that there was an intrinsic muscle abnormality in CRPS. This was obvious even to me without a formal training in muscle sonoanatomy.
Normal muscle on USG has clearly delineated muscle outlines and looks generally black with bright streaks of connective tissue framework that holds the muscle fibers in well-defined bundles. (fig 15) In stark contrast, the CRPS muscles in this patient looked like a sheet of barren white (fibrotic) tissue without any form or shape, with no discernible outlines. The bulk of muscle was also very much reduced in CRPS compared to normal muscles.
Figure 14- documentation of co-contraction effects with a dynamometer



The cocontraction of CRPS makes it impossible for the patient to even to retain the bulb of the dynamometer in the palm , let alone grasp it to squeeze it. But after thrice weekly USGDN, the patients are able to grasp the bulb of the dynamometer by 15 days but are usually not able to generate any pressure . But by 30 days, most of them can generate about 3pound /square inch pressure which is sufficient power to perform all daily activities of life .
Figure 15 CRPS in a 26-yr-old after metacarpal fracture 18 months prior

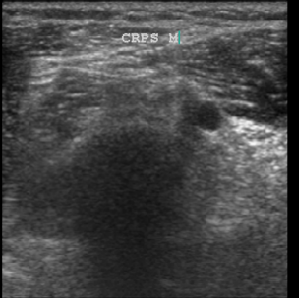

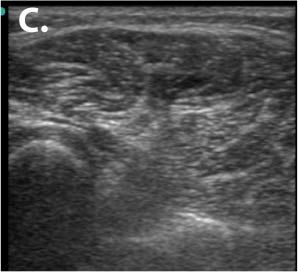
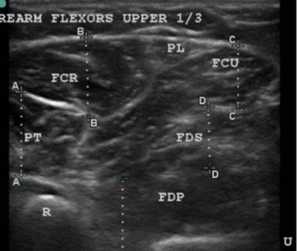
Row 1- The ultrasound appearance of a normal muscle from the healthy limb. Note that the outlines of the muscles are clearly defined by shiny white borders and all the different muscles are identifiable and can be named. The muscles themselves have a dark background within a framework of supporting fibrous tissue which appears like shiny white streaks, and this is the typical sonographic signature of muscle. The second image shows her hand trying to make a fist, that she is unable to flex the fingers onto the palm or touch the tips of fingers to each other or thumb. Ultrasound of the CRPS limb in the 3rd image shows that there is no definition of muscle boundaries nor is there the normal contrast of black muscle in with white streaks of fibrous framework in between as compared to the ultrasound of the muscles of normal limb. In short there is a complete disruption of muscle structure.
2nd row- The first image shows that the patient has regained the ability to make a fist after 1month of USGDN of the forearm muscles. The patient opening the cap of a bottle 18 days after treatment which was impossible for her before USGDN at Ashirvad. Image C shows the return of normal structure to the muscles on ultrasound although there is still some predominance of fibrosis in the form of hyperechogenic fibrous streaks.
We found that these ultrasound changes of muscle structure disruption were consistently present in varying degrees in every patient that we examined thereafter. The USG changes of muscle abnormality appear as early as 15 days after the onset of CRPS and continue to be not just present but keep worsening till the muscle becomes completely fibrotic as indicated by the white-out appearance in all muscles affected by CRPS of medium or long duration. This was the picture that we saw in the first patient who had CRPS for 2 years. Subsequently we made it a part of our CRPS management protocol to routinely to document the muscle changes in every patient before USGDN, at 15 and 30 days and after the patient has recovered fully and correlate it with documentation of clinical findings.
We document all the clinical findings of the patients before and after treatment. This includes still and videos of their movement limitations as well as objective documentation of the pressures that they can generate with their fisted hand (dynamometer) and fingers with pinch gauge (figures 9,12,14) The range of motion (ROM) at all the joints of the limb are documented with a goniometer. The function of the limb is documented with the disability of the arm hand and shoulder (DASH) score. (74) USG documentation included both still images and videos of resting muscles, as well as the sequence of events on needle introduction observed on USG.
One interesting finding of doing serial USG was that USGDN seemed to bring back black islands of muscle in the white fibrotic tissue. The reappearance of muscle coincided with the return of movements executed by that muscle in the stiff hand. This meant that USGDN was actually making the muscle fibers to regenerate amongst the residual connective tissues (figure 16).
How and why this muscle changes occurred was still a mystery, but the documentation went on both of USG, and the variety of clinical presentations. This systematic documentation was crucial to the acceptance of our findings by the scientific community and for us to publish our unusual findings in CRPS with a safe and effective treatment like USGDN in reputed international journals. Our first article “Ultrasound Appearance of Forearm Muscles in Eighteen Patients with Complex Regional Pain Syndrome Type -1 of the Upper Extremity” was provisionally accepted in 2011 but was finally published in 2012 and the printed version came out in January 2013 edition of the journal Pain Practice. (51)
One of the reasons for this long delay was that the topic straddles the 2 specialties, pain medicine and ultrasonography. The reviewers were pain specialists who had no expertise in diagnostic applications of USG even though they might have used USG to perform their interventions. The actual experts in ultrasonography have no experience with CRPS. We had accidentally stumbled into a highly rarified area because of our work involved with two diverse topics, CRPS and diagnostic USG.



